CDC: Monkeypox Causing Severe Infections, Test Patients for HIV
By Gary Evans, Medical Writer
A severe spectrum of monkeypox disease is appearing in patients with untreated human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS), prompting the Centers for Disease Control and Prevention (CDC) to urge HIV testing for patients with monkeypox.
“During the current outbreak in the United States, 38% of people diagnosed with monkeypox were coinfected with HIV, and most reported cases of monkeypox with severe manifestations have been among people living with untreated HIV,” the CDC stated in a recent health advisory.1 “Because people with HIV-associated immunocompromise are at risk for severe manifestations of monkeypox, the HIV status of all sexually active adults and adolescents with suspected or confirmed monkeypox should be determined.”
Although severe cases of monkeypox can manifest in those immunocompromised for other reasons, and even the immunocompetent, the CDC clearly is concerned about the intersection between the emerging pox virus and HIV/AIDS. Many people may not know their HIV status or have stopped effective available treatments to suppress the retrovirus.
“The majority with advanced HIV disease are not virally suppressed, with a low CD4 cell count of below 200, and many below 50 — indicating substantial immunosuppression,” Agam Rao, MD, a CDC epidemiologist, said at a clinical briefing.
Treatment should include optimizing immune function, limiting immunosuppressive medications if not otherwise indicated, and providing antiretroviral therapy for people with HIV, the CDC recommended.
HIV coinfection with monkeypox — particularly for those who have low CD4 counts — has produced devastating infections of disseminated monkeypox infection. A clinician who reported the first U.S. monkeypox death said that, on autopsy, the virus was found in bone marrow and in the brain, since it had disseminated widely throughout the body.
The presentation of disease was similar to that once seen in the hemorrhagic stage of smallpox, a rare but usually fatal variety of that vanquished virus, said Jemma Alarcón, MD, MPH, a CDC Epidemic Intelligence Service officer in Los Angeles.
“This was the first confirmed monkeypox-related death in the United States, occurring in a 33-year-old man with HIV/AIDS with a CD4 [count of] 35 cells/mm,” she said at the CDC clinical briefing. “[He] died from disseminated monkeypox, despite treatment with 28 consecutive days of oral tecovirimat.”
Two other U.S. patients with monkeypox have died, but there is some ongoing investigation into whether the virus was the cause of death in one case.
Opioids Cannot Stop Pain
Alexandra Dretler, MD, an infectious disease physician at Emory University Hospital in Atlanta, described another case report of a severely infected patient who had survived as of the Oct. 6, 2022, briefing.
The patient is a man in his 30s with known HIV. He had not been taking antiretroviral therapy for six months, and his CD4 count had fallen below 200.
“He reported recent sex with a man, after which he developed multiple penile and other scattered lesions consistent with monkeypox,” Dretler said at the briefing. “He had severe and really persistent pain from the penile lesions that was making it impossible to sleep or really get any relief despite getting oral opioids.”
The patient was admitted and subsequently discharged on a 14-day course of oral tecovirimat. Ten days later, he was readmitted with multiple lesions on the body, genitals, and one eyelid. He also had a combination of severe pain, weight loss, malaise, and weakness.
“Some patients with monkeypox in the United States have experienced prolonged hospitalizations, substantial morbidity and deaths have occurred,” said Caroline Schrodt, MD, MSPH, lead of the CDC clinical escalations team.
Manifestations of these cases include an atypical or persistent rash, as well as coalescing and necrotic lesions, she said at the briefing.
“Some of these have required extensive surgical debridement or amputation of an affected extremity,” Schrodt said. “Lesions on a significant proportion of the total body surface area may be associated with a secondary bacterial or fungal infection.”
Lesions may be in sensitive areas, including mucosal surfaces, such as the oropharynx, urethra, rectum, or vagina, “resulting in severe pain that interferes with activities of daily living,” she said. Bowel lesions that can cause significant tissue swelling can lead to obstruction. Airways also can be obstructed, and oropharyngeal lesions can inhibit oral intake.
Severe monkeypox can have a necrotizing effect that kills underlying tissue. It can affect multiple organ systems and cause neurologic conditions, such as encephalitis.
Thus far, the cases of severe monkeypox have been in men. However, people who are immuno-compromised (e.g., cancer) pregnant, young children under 8 years of age, and people with atopic dermatitis or eczema are at risk of severe monkeypox if infected. Most of these severe patients have progressive illness, sometimes with greater than 100 lesions, with new lesions appearing despite treatment.
The CDC monkeypox alert included the following recommendations for healthcare providers:
• Upon initial presentation of signs and symptoms consistent with monkeypox, in addition to monkeypox, test all sexually active adults and adolescents for HIV (including acute infection) and other sexually transmitted infections (such as syphilis, herpes, gonorrhea, and chlamydia), and assess for other immunocompromising conditions.
• Be familiar with severe manifestations of monkeypox and risk factors for severe disease.
• Consider treating immunocompromised people diagnosed with monkeypox with tecovirimat early in the course of disease and consider a prolonged course of tecovirimat for those with more refractory and severe monkeypox infection.
• Have a low threshold to use multiple medical countermeasures, including tecovirimat, cidofovir, or brincidofovir, and vaccinia immune globulin intravenous (VIGIV) in immunocompromised people who present with severe manifestations of monkeypox or are at high risk of progression to severe manifestations.
• Discuss HIV pre-exposure prophylaxis (PrEP) with those who are HIV negative and at risk for HIV.
Stopping Hospital Transmission
As patients with severe monkeypox are admitted and readmitted to hospitals, infection control rigor and compliance is critical to protect patients and healthcare workers.
Jill Holdsworth, CIC, FAPIC, outlined some of the key infection control measures for monkeypox at a recent webinar held jointly by the Association for Professionals in Infection Control and Epidemiology (APIC) and the Society for Healthcare Epidemiology of America (SHEA).
“As always, we’re going to continue to say identify, isolate, and inform,” said Holdsworth, manager of infection prevention at Emory University Hospital Midtown. “That’s what we always want to really focus on when we’re talking about infection prevention with any type of infectious disease.”
Patients with a new vesicular and pustular rash are easier to identify and begin a monkeypox workup for, but also be aware of “unexplained” conditions, she said.
“One of the things that we want to really stress is if you’re looking at a patient that might have unexplained pharyngitis or proctitis, really think about what are their risk factors,” Holdsworth said. “We could have exposures if we don’t consider these patients as well. Really think about how you’re going to identify that portion with patients that maybe don’t have lesions or a rash yet.”
The current isolation guidelines call for placement of monkeypox patients in a private room with an unshared toilet, keeping the lesions covered as much as possible. Negative pressure or airborne precaution rooms are not necessary unless an aerosolizing procedure is performed. Healthcare workers entering the room should wear N95 respirators, gowns, gloves, and eye protection. Transmission can occur through skin-to-skin contact and direct or indirect contact with body fluids and respiratory droplets, and suspended droplet nuclei.
“Also, make sure we have a mask on that patient,” she said. “Make sure they’re in a private room with the door closed, cover those lesions whenever possible, and limit movement in and out of the room.”
Monkeypox patients can be infectious up to five days before onset of rash. “We know that they are infectious until there’s that new skin growth that’s coming up after those lesions have crusted,” Holdsworth said. “That duration of isolation is really important to understand.”
Part of that informing function is signage on doors and alerting appropriate staff who may enter the room. “A lot of people tell me that they were using their COVID signs, and they just made them look a little bit differently so that they were more visible as monkeypox,” she said.
Informing also includes first responders or other staff who may have brought the patient in or seen them without personal protective equipment (PPE). “If the patient comes through the emergency room or by ambulance, how are you making sure that you have that communication back to personnel who are supervising that unit?” she said. “[Inform] anyone who is taking care of the patient on that unit, infection prevention, public health — make sure that you cover all of your bases.”
Since monkeypox can spread by clothing or sheets, hospital linen has to be handled with caution as an environmental concern.
“Linen does not just mean bed sheets, it also means towels, it also means clothing,” she said. “One thing that is very specific on the CDC website is you don’t want to shake or handle linens in a way that disperses infectious material. You don’t want to be flapping the sheets around, you don’t want to be throwing the towels around the room.”
Instead, handle these items carefully, contain them in a linen bag as soon as possible and make you are wearing PPE, she said. “You want to make sure that your environmental services personnel are comfortable, trained with PPE, wearing the PPE correctly, so that when they are cleaning the room, that they are doing so in a safe manner and that they know all of these things as well.”
Communicate these concerns to laundry personnel in-house or the service used by the hospital “so it is a partnership and a collaboration with your linen companies and environmental services, so if they are the ones who are handling the linen, too,” Holdsworth says.
Continuing with environmental concerns, trash from monkeypox rooms should be treated as regulated medical waste, “meaning the same as other potentially infectious materials that you use for isolation and other things,” she said. As bad as the monkeypox outbreak has been, it could be worse in the area of medical waste. As of Sept. 28, 2022, the CDC clarified that the infections in the current outbreak are from Clade II, the generally milder form of the virus formerly called West African. Clade I monkeypox (formerly Congo Basin) requires more rigorous treatment and handling of medical waste. The geographic location names were changed to numbers to prevent stigma.
In terms of cleaning environmental surfaces, use a product on the Environmental Protection Agency Q list with an “emerging viral pathogens claim,” Holdsworth said. “Follow the manufacturer’s instructions for use and, as always, make sure that you’re using something that is going to be easy to use and to be compliant during use,” she said. “You want to avoid things like dry dusting, sweeping, vacuuming. Using wet methods of cleaning is always going to be better for things like this.”
It is important that infection control work closely with environmental services, making sure they know how to use the product and use appropriate PPE.
“Really working with them in partnership is what has worked best for a lot of people I’ve talked to, because everybody’s nervous,” she said. “Everybody was a little scared in the beginning, just to clean these rooms, so really help people understand how to do this safely and emphasize that PPE works.”
Reassuring Data
Although vigilance with infection control still is critical, a recent study by Colorado public health investigators concluded that the risk of healthcare workers acquiring occupational monkeypox is “very low.”2 They followed more than 300 medical staff that cared for patients who were later determined to have monkeypox.
Healthcare workers were assessed for risk and actively monitored for 21 days when indicated. None acquired monkeypox, but the caveat is that some received post-exposure prophylaxis (PEP) that could have prevented infection. There was a clear need for infection control education, since many of the healthcare workers were not wearing the recommended PPE for monkeypox.
“During May 1-July 31, 2022, a total of 313 healthcare personnel (HCP) interacted with patients with subsequently diagnosed monkeypox infections while wearing various combinations of PPE,” investigators reported. “[Only] 23% wore all recommended PPE during their exposures. Overall, 28% of exposed HCP were considered to have had high- or intermediate-risk exposures.” (See Figure 1.)
Figure 1. Healthcare Personnel (HCP) Risk Classification Flow Chart for Monkeypox |
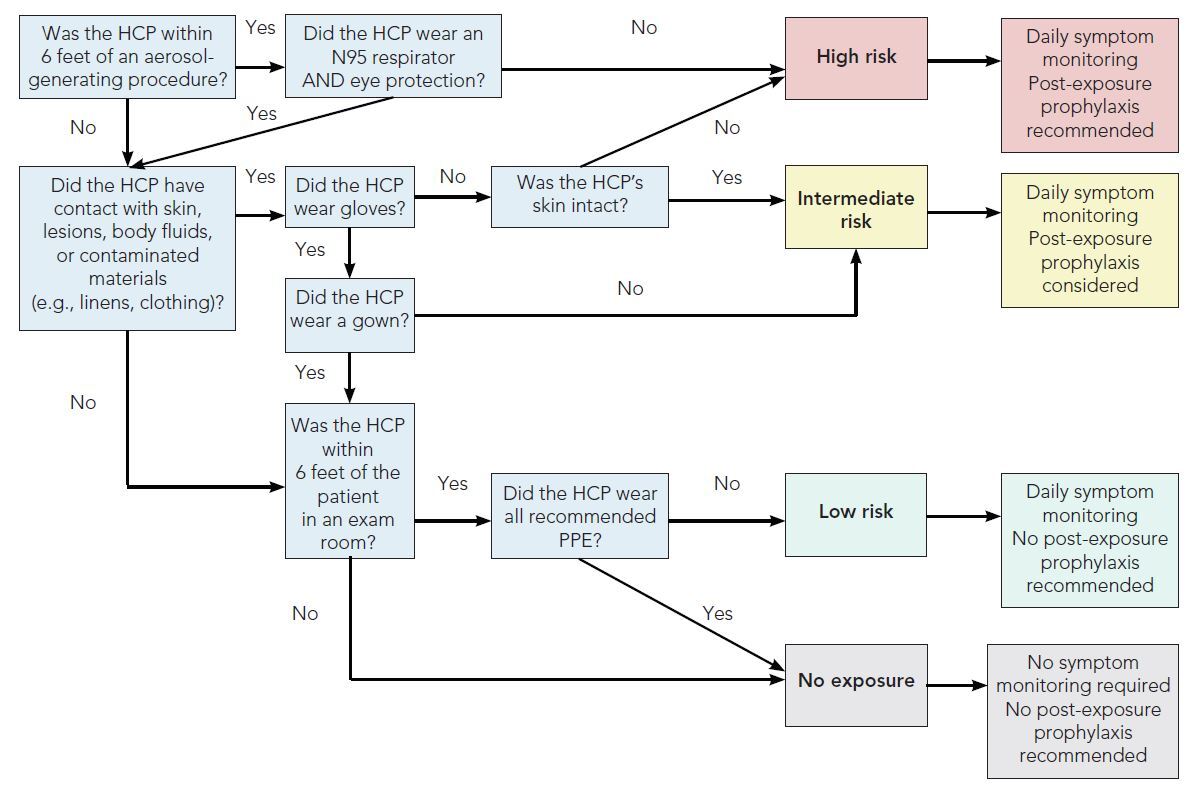 |
Note: Bloodborne pathogen exposure (splashes or needlestick injuries) should automatically be considered high risk exposures. Source: Colorado Department of Public Health & Environment. Monkeypox resources for health care providers. https://cdphe.colorado.gov/diseases-a-to-z/monkeypox-resources-for-health-care-providers Healthcare personnel (HCP) risk classification flow chart for monkeypox: https://drive.google.com/file/d/1Oss8Ii9jynYFfgSK3Op9GXp8MqaCk-nw/view |
These high and intermediate exposed workers were offered PEP with the Jynneos vaccine. “Among eligible HCP, 37 (43%) received PEP, including 10 (50%) with high-risk exposures and 27 (40%) with intermediate-risk exposures,” the authors said.
Hospital Infection Control & Prevention asked for further comment on the study from lead author Kristen Marshall, PhD, MPH, an epidemiologist at the Colorado Department of Public Health and Environment (CDPHE) in Denver.
HIC: Just to clarify, in the healthcare workers who were administered PEP, we do not know if they would have developed an infection or not?
Marshall: Correct, we do not know if healthcare workers would have developed an infection had PEP not been given.
HIC: Was PEP given as a single shot regimen or separated into two shots?
Marshall: PEP has been administered as both a single- and two-dose series. Jynneos is a two-dose vaccine meant to be administered 28 days apart. Due to rapidly rising cases and an extremely limited federal supply of vaccines, Colorado temporarily implemented a strategy prioritizing first doses to provide early protections to as many at-risk Coloradans as possible. There is no maximum allowable interval between the first and second doses of a Jynneos vaccine series, and the second dose can be safely administered after the recommended 28-day window without restarting the vaccination series. CDPHE contacted people who received their first dose and provided contact information to inform them that second doses are now available statewide.
HIC: Can you comment on the lack of full compliance with PPE in many exposures? Could this be an aspect of pandemic fatigue?
Marshall: Ultimately, the data did not capture why there was a lack of full compliance with recommended PPE for monkeypox.
Monkeypox is a condition that most healthcare providers in Colorado had not previously seen, and many people have presented with symptoms different than in previous monkeypox outbreaks. Especially early in the outbreak, healthcare providers may not have worn all recommended PPE because they did not recognize that a patient with symptoms might have monkeypox. Healthcare workers also might not have been aware of community transmission, or they might not have been aware of the current PPE recommendations during care for monkeypox patients.
Additionally, patients may have been unaware that they had monkeypox or had been exposed and may not have notified their healthcare provider about relevant signs or symptoms before their arrival or during their visit to ensure that recommended infection prevention and control measures were used. Infection prevention and control training for all healthcare workers is important in all healthcare settings.
HIC: In light of reporting no transmission to HCP, is it still important — perhaps more important than ever — to emphasize full PPE compliance with a suspected or confirmed monkeypox case?
Marshall: While monkeypox transmission in healthcare settings is rare, it is important for healthcare workers to take proper infection control, including donning proper PPE and practicing good hand hygiene. PPE should include gown, gloves, eye protection, and National Institute for Occupational Safety & Health (NIOSH)-approved respirator with N95 or higher filters.
Editor’s note: Infection preventionists needing more information on severe monkeypox cases can contact the CDC Monkeypox Response Clinical Escalations Team via email: [email protected]. Healthcare providers may contact the CDC Emergency Operations Center at (770) 488-7100 for multidisciplinary consultation with specialists, such as infectious disease, ophthalmology, dermatology, urology, or critical care medicine.
REFERENCES
- Centers for Disease Control and Prevention. Severe manifestations of monkeypox among people who are Immunocompromised due to HIV or other conditions. Published Sept. 29, 2022. https://emergency.cdc.gov/han/2022/han00475.asp#:~:text=If%20you%20are%20someone%20with,monkeypox%20from%20a%20healthcare%20provider
- Marshall KE, Barton M, Nichols J, et al. Health care personnel exposures to subsequently laboratory-confirmed monkeypox patients — Colorado, 2022. MMWR Morb Mortal Wkly Rep 2022;71:1216–1219.