What Kind of Artifact?
By Ken Grauer, MD
Professor Emeritus in Family Medicine, College of Medicine, University of Florida
To emphasize the importance of recognizing the clinical finding shown in the figure, no history is given. The two most helpful leads for interpretation of these unusual ECG findings are lead I and lead V3. How would you interpret this tracing?
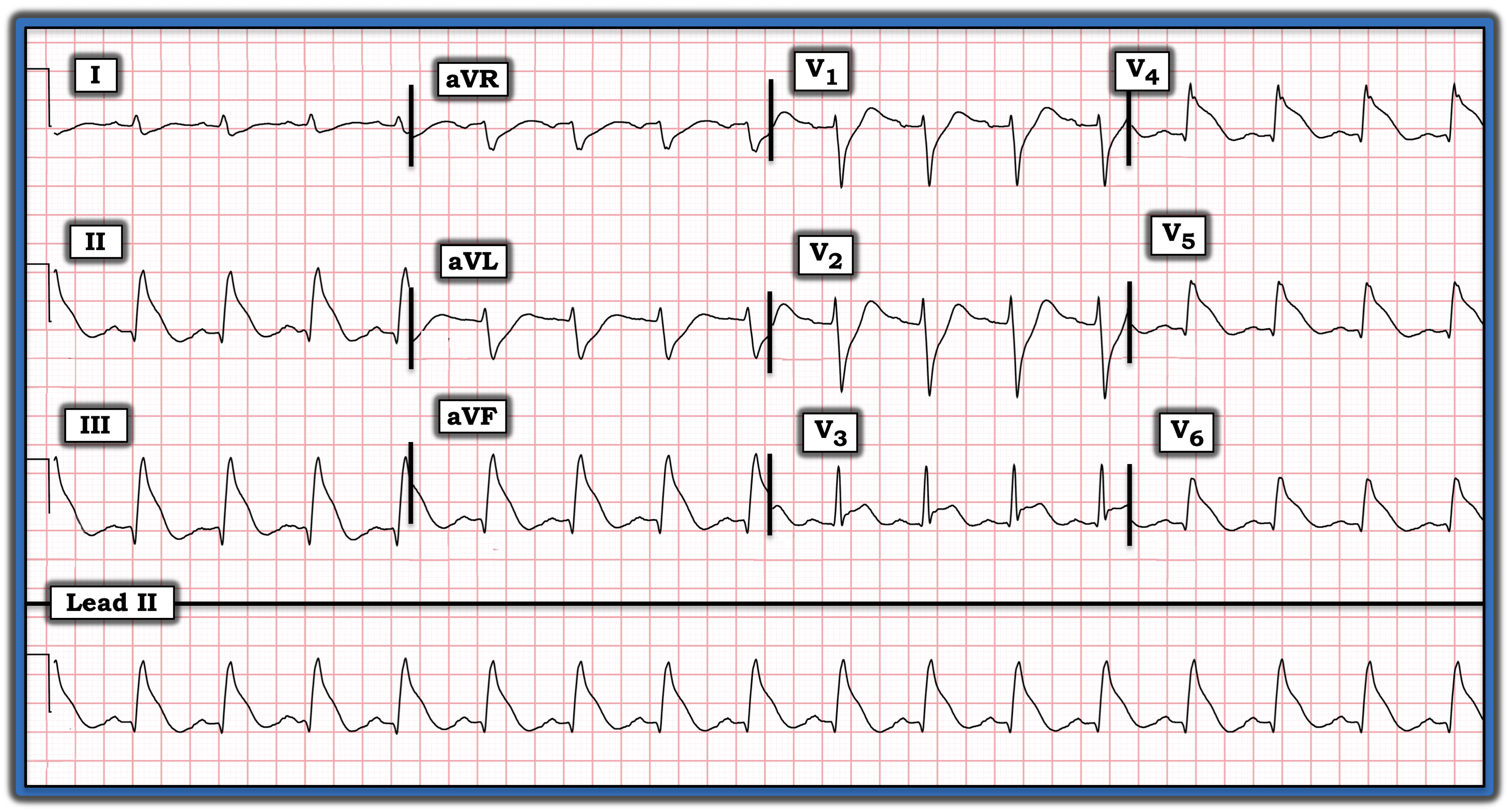
Interpretation: Despite our initial impression of profound QRS
widening, it turns out that the QRS is not wide at all. There is no artifact. Instead, there is marked ST-segment elevation in multiple leads. The underlying rhythm in this case is sinus, as determined by the presence of distinct upright P waves in each of the inferior leads (as well as the presence of definite P waves with a constant PR interval in each of the chest leads).
- The most challenging aspect of this tracing is determination of QRS duration. The QRS complex looks to be very wide in multiple leads because there is no distinct border between the end of the QRS and the beginning of the ST segment in either those leads showing marked ST elevation (i.e., leads II, III, aVF, and V4, V5, and V6), nor in those leads with marked ST depression (i.e., leads aVL, V1, and V2).
- The key is to look for the one or two leads in this 12-lead tracing in which you can confidently identify the end of the QRS complex. Both the shallow S wave in lead I and the elevated but sharply defined S wave in lead V3 allow you to do so.
- Since leads II and III and leads V1 and V2 are simultaneously-recorded with lead I and lead V3, respectively, drawing a vertical line down from the end of the S wave in lead I and up from the end of the elevated S wave in lead V3 allows you to define the “true” end of the QRS complex in each of these leads.
- Now that you know the point that marks the end of the QRS complex in lead II you can draw a vertical line up from this “true” end point in the long lead II rhythm strip to define the beginning of the ST segment in simultaneously recorded leads aVL and aVF and in leads V4, V5, and V6.
Bottom Line: This rhythm is sinus. The QRS complex is not wide. Instead, the dramatic ST elevation in inferior and lateral chest leads (called “shark fin” ST elevation because of its shape) — in association with marked ST depression in leads aVL, V1, and V2 — suggests extensive acute infarction. It turns out that today’s patient presented with new chest pain and was found to have severe multivessel disease with acute occlusion of a major coronary vessel.
For more information about and further discussion of this case, please visit https://tinyurl.com/KG-Blog-353
To emphasize the importance of recognizing the clinical finding shown in the figure, no history is given. The two most helpful leads for interpretation of these unusual ECG findings are lead I and lead V3. How would you interpret this tracing?
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.