
What Are Those T Waves?
By Ken Grauer, MD
Professor Emeritus in Family Medicine, College of Medicine, University of Florida
The patient whose ECG appears in the figure presented to an ambulatory care clinic for chest pain. Is the patient likely to have hyperkalemia?
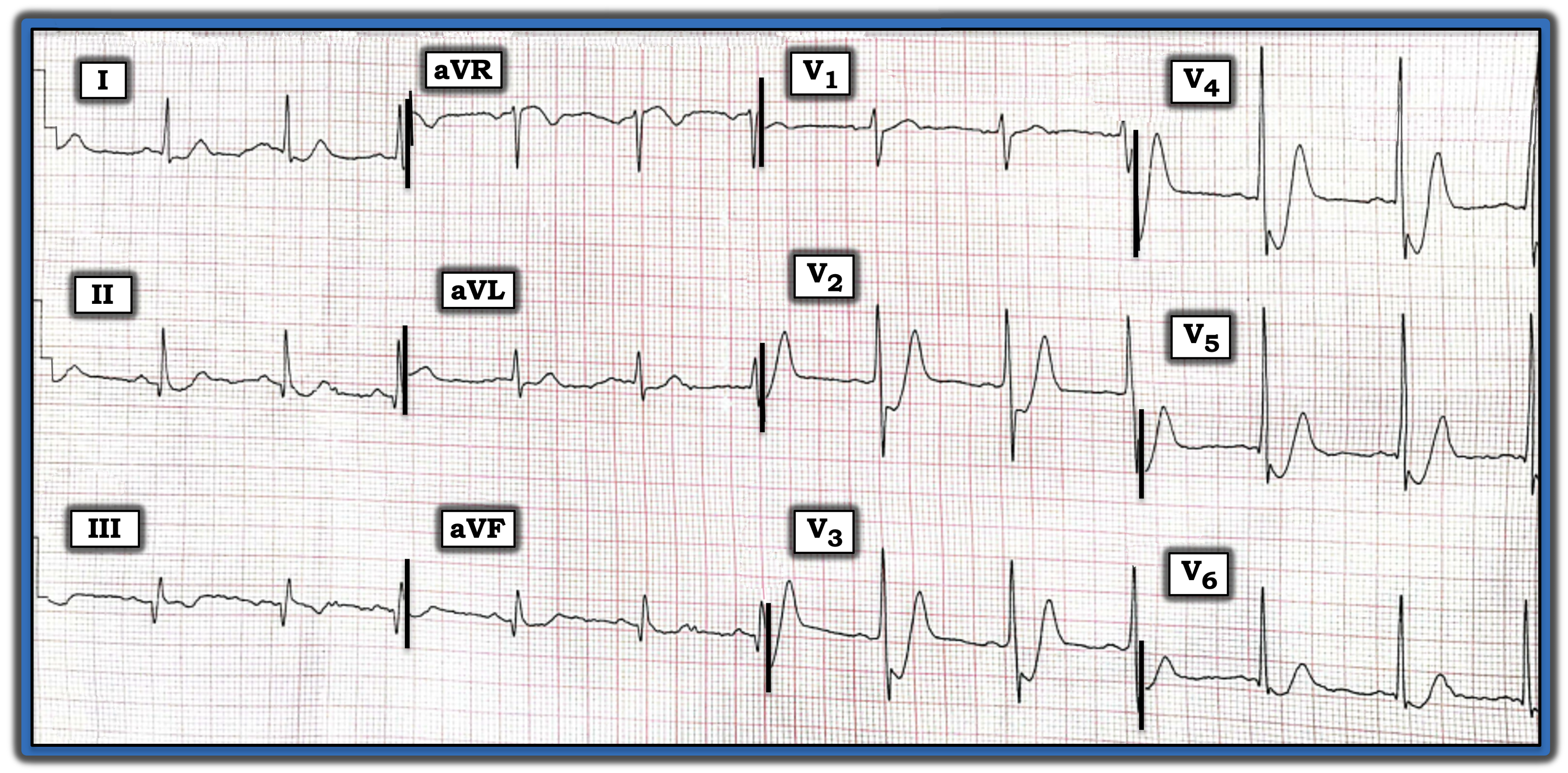
Figure: ECG from a patient with chest pain.
INTERPRETATION
Today’s ECG is markedly abnormal.
- The upright P waves in lead II define the rhythm as sinus, here at a rate of ~70/minute. Intervals and the frontal plane axis are normal. There is no chamber enlargement.
- Relatively large Q waves of uncertain significance are seen in the inferior leads. This may represent prior inferior infarction, but this finding is probably not recent or acute. Small, septal q waves are seen in lateral chest leads.
- R wave progression is marked by early transition with a predominant R wave already by lead V2.
The most remarkable finding is the marked downsloping ST depression, followed by tall, peaked T waves with a relatively narrow base in leads V2 through V5.
- Although verifying serum potassium is clearly indicated, I would suspect that this patient does not have hyperkalemia because: a) There is marked J-point ST depression in each of the chest leads with T wave peaking, which is not a typical finding with hyperkalemia; and b) There is no indication of any T wave peaking in any of the limb leads (whereas T wave peaking with hyperkalemia tends to be generalized).
- Against acute posterior infarction is the presence of these ST-T wave changes in virtually all chest leads, whereas posterior infarction is unlikely to manifest such profound ST depression simultaneous with such tall, peaked T waves in so many chest leads.
BOTTOM LINE
Given the presence of chest pain, it seems likely that the diffuse J-point ST depression seen in today’s tracing, in association with these large, peaked chest lead T waves, represents some variation of deWinter T waves, indicative of acute left anterior descending) coronary artery occlusion. The patient was treated promptly with thrombolytic therapy.
For more information about and further discussion of this case, please visit: https://tinyurl.com/KG-Blog-340
The patient whose ECG appears in the figure presented to an ambulatory care clinic for chest pain. Is the patient likely to have hyperkalemia?
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.