By Ken Grauer, MD
Professor Emeritus in Family Medicine, College of Medicine, University of Florida
The ECG in the figure below was recorded on a patient with new chest pain that began one hour earlier. How would you interpret this ECG? Should the catheterization lab be activated, given the history and this ECG?
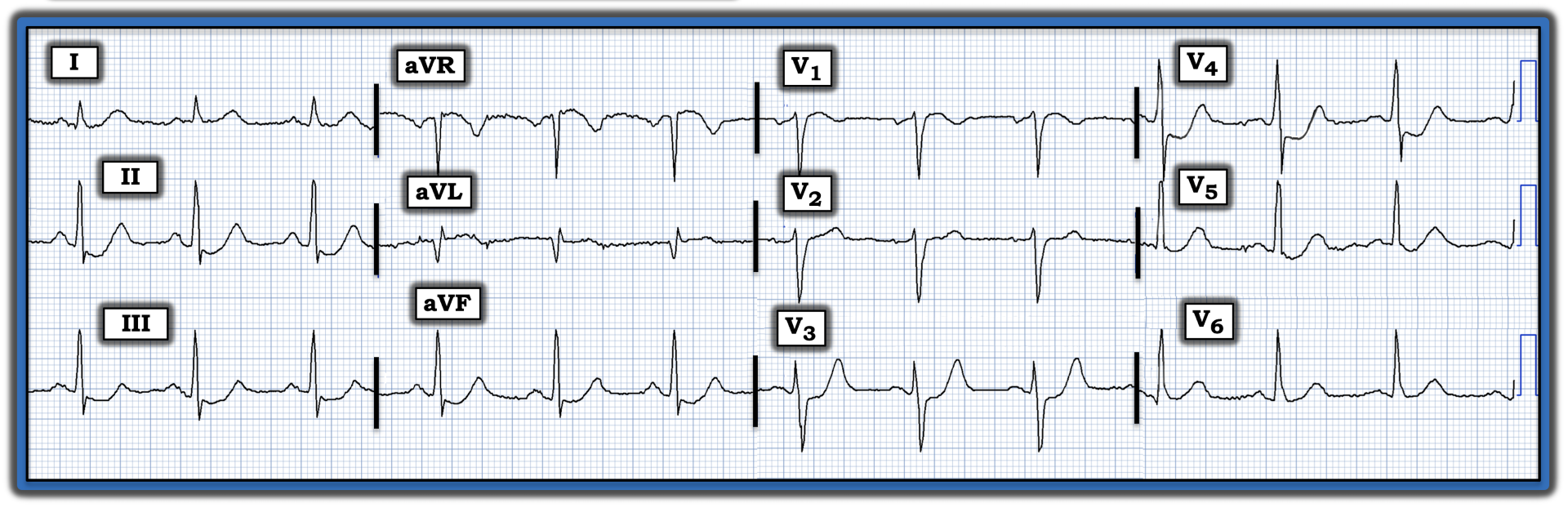
Interpretation: In view of the history in this case, the ECG in the figure is extremely worrisome. The rhythm is sinus at ~75 beats/minute. Intervals and the axis are normal. There is no chamber enlargement. R wave progression is normal.
• The most concerning aspect of this ECG is the ST depression visible in no less than six leads — including the inferior leads (II, III, aVF) — and in leads V3 through V5. ST depression in each of these leads is marked by terminal T wave positivity, which is a sign of ischemia. This amount of ST depression in so many leads, in association with the ST elevation that we see in lead aVR (and also slightly in lead V1), suggests diffuse subendocardial ischemia, with a high likelihood of significant underlying coronary disease.
• Of special concern in this tracing is that maximal ST depression is visible in lead V4, which manifests a “shelf-like,” if not slightly downsloping, shape of ST depression. When the amount of ST depression is maximal in lead V2, V3, or V4 in a patient with new chest pain, this picture is highly suggestive of acute posterior infarction in need of prompt cardiac catheterization with coronary reperfusion.
Additional ECG findings of note in this tracing include:
• The ST segment in lead V2 is flat. Normally, there is slight, gently upsloping ST elevation in leads V2 and V3, such that this ST segment flattening without any elevation in lead V2 clearly is abnormal.
• Lead aVL manifests a large Q wave and subtle-but-real ST elevation.
Bottom line: Cardiac catheterization was performed promptly on this patient, revealing diffuse underlying coronary disease, with acute occlusion of the first obtuse marginal branch of the left circumflex artery. A stent was placed, and the patient fared well.
• These findings on cardiac catheterization are consistent with this ECG in that there was diffuse coronary disease with acute inferolateral infarction.
NOTE: For more information about and further discussion of this case, please visit: https://tinyurl.com/KG-Blog-351.
The ECG in the figure was recorded on a patient with new chest pain that began one hour earlier. How would you interpret this ECG? Should the catheterization lab be activated, given the history and this ECG?
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.