The Silent Epidemic: Hepatitis C Virus
EXECUTIVE SUMMARY
Hepatitis C is transmitted through contact with infected blood. The degree and severity of infection ranges from mild and self-limiting to severe, fulminant liver failure. Although a person might survive the acute infection with hepatitis C, this virus can progress to a chronic infection, occurring in up to 70% of infected individuals no matter the timing of infection.
- For the past 30 years, the incidence of liver cancer, the fourth leading cause of cancer mortality, has been rising and is estimated to do so until 2030.
- Hepatitis C accounts for a significant burden of disease. In 2018, Medicare spent more than $4.5 billion on the treatment of hepatitis C in the United States. On a larger scale, the cost of treating the nearly 3.7 million chronically infected patients would exceed $310 billion, with each patient requiring $84,000 of resources.
- The incidence of hepatitis C virus (HCV) has more than doubled since 2013 and continues to rise, with the highest acute infection rates among men and women aged 20-39 years.
- As the result of chronic infection and inflammation, up to 20% of patients with chronic HCV will develop cirrhosis. Further, those who develop cirrhosis have an increased risk of developing hepatocellular carcinoma (HCC). The incidence of HCC in this patient population also increases with age since the risk of development of HCC in a cirrhotic HCV patient is 3% to 8% annually.
- Current recommendations by the U.S. Preventive Services Task Force call for universal screening of HCV. This includes one-time screening of all adults (aged 18 years and older), as well as preconception testing with each pregnancy.
- Routine periodic testing is recommended for those with ongoing risk factors, such as injection drug use, and for patients undergoing hemodialysis.
- Screening is done via hepatitis C antibody (anti-HCV) by enzyme immunoassay and recombinant immunoblot assay. After a positive anti-HCV has been obtained, a confirmatory test is completed by measuring the hepatitis C viral load. Viral load is measured using the HCV ribonucleic acid (RNA) polymerase chain reaction assay.
- The primary goal of treatment is to achieve sustained virologic response (SVR) or undetectable viral load at 12 weeks.
- In patients with advanced fibrosis or cirrhosis, subspecialty care may be required, especially for those eligible for consideration for liver transplantation because of hepatic decompensation.
- The presence of cirrhosis needs to be assessed. This can be performed by calculating a fibrosis index based on the four-factor Fibrosis-4 (FIB-4) score based on liver enzymes and platelet count.
- For patients with hepatitis B virus (HBV) coinfection: In those without cirrhosis, treatment should be offered if alanine transaminase is more than twice the upper limit of normal and the patient has an elevated viral load (HBV deoxyribonucleic acid [DNA] > 2,000 IU/mL if HBV e antigen-negative and HBV DNA > 20,000 IU/mL if HBV e antigen-positive).
- If the patient has not had HCV genotype testing, they should be started on sofosbuvir (400 mg)/velpatasvir (100 mg) (brand name: Mavyret) for 12 weeks or glecaprevir (300 mg)/pibrentasvir (120 mg) (brand name: Epclusa) for eight weeks. These should be used in patients without cirrhosis or previous treatment for HCV.
- In patients with decompensated cirrhosis, defined as having a Child-Turcotte-Pugh score of ≥ 7, their treatment regimen is more complicated. Because of their disease progression and resulting hepatic impairment, they should be referred to a liver transplant center.
- Treatment monitoring in patients diagnosed with HCV depends largely on each patient’s response to antiviral therapy. Patients ultimately can be divided into two groups, those who have achieved SVR and those who have not. SVR is defined as undetectable RNA 12 weeks after the completion of antiviral therapy. With this definition in mind, obtaining an HCV quantitative, full-time PCR (HCV RNA quant) at the 12-week post-therapy mark is recommended.
- HCV can be treated by a patient’s primary care physician; in fact, the Centers for Disease Control and Prevention encourages family physicians to treat hepatitis C. When primary care physicians prescribe direct-acting antiviral drugs, specifically to patients with uncomplicated hepatitis C, outcomes are comparable to those seen with subspecialists. Primary care health professionals are the first line of medical practitioners. This group is instrumental in screening for and treating hepatitis C.
Viral hepatitis, most commonly caused by hepatitis A, B, and C, is an infection of the liver. As of 2020, it is estimated to be acquired by a little more than 100,000 Americans yearly.1 Hepatitis C is transmitted through contact with infected blood. The degree and severity of infection ranges from mild and self-limiting to severe, fulminant liver failure.2 Although a person might survive the acute infection with hepatitis C, this virus can progress to a chronic infection, occurring in up to 70% of infected individuals no matter the timing of infection.3
Over time, chronic infection with hepatitis C virus (HCV) can progress to more severe liver disease. Long-term infection and inflammation results in cirrhosis and can predispose these patients to hepatocellular carcinoma. For the past 30 years, the incidence of liver cancer, the fourth leading cause of cancer mortality, has been rising and is estimated to do so until 2030. Hepatocellular carcinoma (HCC), the most commonly diagnosed liver cancer, accounting for up to 70% to 80% of diagnoses, has been associated with chronic hepatitis C infection in up to 90% of cases, depending on global region.4
Although some hepatitis viruses have vaccinations, this is not the case with hepatitis C because of the high variability of this virus. HCV has been shown to have up to seven distinct genotypes, with up to 60 different subtypes, that are consistently mutating. Even within an individual with HCV infection, multiple closely related variants are produced, leading to continued infection that seems to be one step ahead of previously produced antibodies.5 This virus’ extensive mutation and variability has proved making an effective vaccination quite difficult and unsuccessful to this point.6
Given its high propensity to result in chronic infection requiring long-term treatment, hepatitis C accounts for a significant burden of disease. In 2018, Medicare spent more than $4.5 billion on the treatment of hepatitis C in the United States. On a larger scale, the cost of treating the nearly 3.7 million chronically infected patients would exceed $310 billion, with each patient requiring $84,000 of resources for a 12-week course of treatment.7 In addition to financial burden, this virus has psychosocial implications as well. The effect of the virus on mental well-being is multifactorial, and up to 50% of those infected may experience cognitive decline and psychological disorders such as depression and fatigue.8 As evident, the effect on the quality of life in persons with chronic hepatitis C infection cannot be understated.
Epidemiology and Morbidity of HCV
HCV has an estimated worldwide prevalence ranging from 0.5% to 2.5% and an estimated incidence of 1.75 million new cases annually.9 Acute infections are difficult to determine, since most are asymptomatic. Seventy percent of acute infections will progress to chronic hepatitis C, the most common cause of viral chronic liver disease in the United States.10
The incidence of HCV has more than doubled since 2013 and continues to rise, with the highest acute infection rates among men and women aged 20-39 years.11 Chronic infection, determined by the presence of anti-HCV antibodies, is seen in more than 2.7 million Americans (almost 1%) , leading to nearly 15,000 HCV-related deaths in 2020.12
Populations at risk of HCV infection include injection drug users (IDU), the incarcerated population, those who received blood/blood product transfusions or organ transplant prior to 1992, patients who received clotting factor prior to 1987, long-term dialysis patients, people with tattoos and piercings (other than ears), healthcare workers with sharp needle or other exposure, infants born to infected mothers, and those with high-risk sexual behavior (multiple partners, sexually transmitted disease [STD] exposures, etc.).13 Regarding transmission, this virus is most commonly transmitted through the sharing of injection equipment during intravenous (IV) drug use but also through use of inadequately sterilized medical equipment and the transfusion of unscreened blood.10 Of note, sexual transmission of this virus does occur, but it is much less frequently transmitted in this manner. Those with multiple sexual partners or those who engage in anoreceptive intercourse also are at an increased risk.14 Additionally, HCV continues to have much higher rates in the incarcerated population, with prevalence estimated to be higher than 15% of the 10.2 million inmates nationally.11
As the result of chronic infection and inflammation, up to 20% of patients with chronic HCV will develop cirrhosis. Further, those who develop cirrhosis have an increased risk of developing HCC. The incidence of HCC in this patient population also increases with age, since the risk of developing HCC in a cirrhotic HCV patient is 3% to 8% annually.11 Other risk factors that predispose patients to this progression include co-infection with hepatitis B, human immunodeficiency virus (HIV) infection, as well as concomitant alcohol use and/or obesity.15 Depending on the region studied, chronic hepatitis infection is implicated in a majority of cases of HCC.16
Screening Recommendations and Rationale
HCV screening recommendations have changed over the decades because of shifting demographics and with the availability of curative therapies. Previously the United States Preventive Services Task Force (USPSTF) recommended screening for HCV for those born between 1945 and 1965. However, as the increase in HCV cases has disproportionately affected younger adults in the setting of the opioid epidemic and rising IDU, the older screening recommendations have been disregarded because they do not include this age group.
Current recommendations by USPSTF call for universal screening of HCV. This includes one-time screening of all adults (aged 18 years and older), as well as preconception testing with each pregnancy. However, this recommendation does not apply to those who reside in a region where the prevalence of HCV ribonucleic acid (RNA)-positivity is less than 0.1%. Prevalence by region can be found on the Centers for Disease Control and Prevention (CDC) website: https://www.cdc.gov/hepatitis/statistics/2021surveillance/hepatitis-c.htm#:~:text=During%202021%2C%2043%20states%20reported,3.45%20deaths%20per%20100%2C000%20people.17-19
Screening for HCV should especially be considered in certain high-risk demographics, including those with conditions or exposures of HIV, IDU (even once), hemodialysis patients, patients with persistently abnormal alanine transaminase (ALT), those who received blood/blood product transfusions or organ transplant prior to 1992, patients who received clotting factor prior to 1987, and children born to HCV-infected mothers. Routine periodic testing is recommended for those with ongoing risk factors, such as IDU, and for patients undergoing hemodialysis. Lastly, it is recommended that any person who requests hepatitis C testing should receive it, regardless of disclosure of risk, since some people may be reluctant to disclose personal information.18
Screening is done via hepatitis C antibody (anti-HCV) by enzyme immunoassay (EIA) and recombinant immunoblot assay (RIBA). The infection can be detected four to 10 weeks after infection and in > 97% of infected persons by six months. After a positive anti-HCV has been obtained, a confirmatory test is completed by measuring the hepatitis C viral load. Viral load is measured using the hepatitis C virus RNA polymerase chain reaction assay (HCV-RNA by PCR). A summary of the screening algorithm is included in Figure 1.17, 19 Many laboratories offer automatic reflex testing based on positive HCV-immunogloblulin G (IgG) testing. Reflex testing can help reduce missed opportunities for confirmatory testing in patients with positive HCV-IgG. This reflex testing has shown excellent sensitivity and specificity with low levels of contamination, suggesting reflex testing to be a valuable option for most patients.
Figure 1. Testing for Hepatitis C Virus |
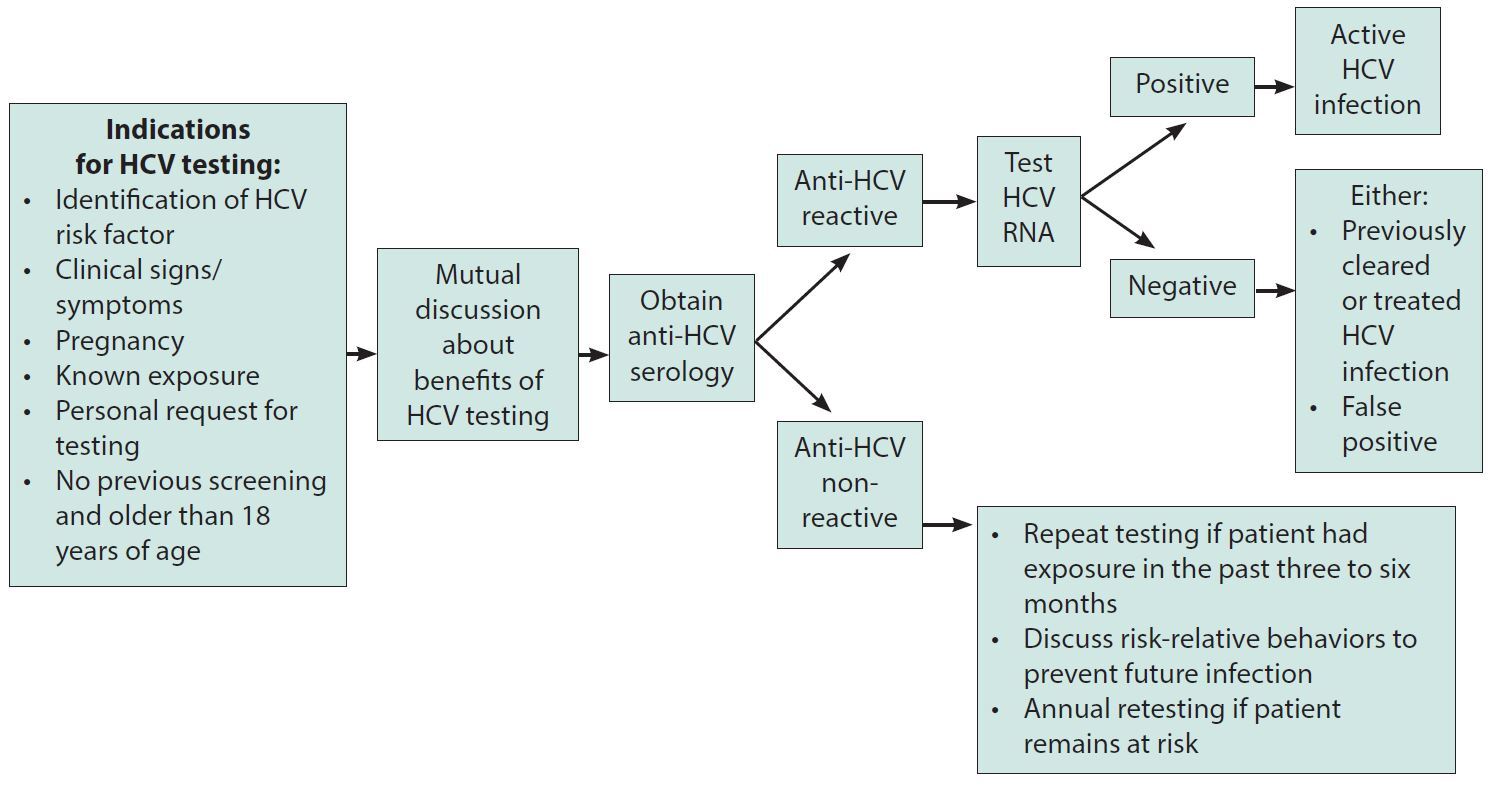 |
HCV: hepatitis C virus; RNA: ribonucleic acid |
In children born to mothers with HCV, testing should be done no sooner than age 18 months, since antibodies from their mother might last until this age. If a diagnosis is desired prior to this time, HCV-RNA testing can be done after the infant’s first well-child visit at 1-2 months of age. This testing should be repeated at a subsequent visit, regardless of the results of such initial testing.19
Outside of disease identification, genotyping in HCV may influence treatment choices. There are six known genotypes and more than 90 subtypes of hepatitis C. While genotyping is not associated with progression of HCV, it is associated with a varying response to current available antiviral therapies.20 The most common, and most aggressive, genotype in the United States is genotype 1, accounting for around 75% of HCV infections.21 Although multiple genotype infection is possible, after a genotype has been identified, subsequent genotyping is not necessary because genotypes do not change over the course of an infection. However, since innovation in antiviral therapy is increasingly pan-genotypic, genotype testing may no longer be required for treatment. 22
Management of HCV
The primary goal of treatment is to achieve sustained virologic response (SVR) or undetectable viral load at 12 weeks.23 The presence of multiple genotypes and numerous subtypes of hepatitis C virus makes targeting treatment difficult.24 However, early recognition and evaluation of active hepatitis C infection can influence treatment selection and consequent prognosis.25
Patients Eligible for Management in the Primary Care Setting
Patients can be managed in the primary care setting with use of the proper tools by primary care providers. Many people living with HCV are undiagnosed, making identification and management in the primary care setting imperative.26 However, many primary care providers are reluctant to treat HCV. Their reasons include the time commitment, lack of education on updated treatment protocols, insufficient tools to educate patients, and lack of insurance coverage and reimbursement.27
According to the American Association for the Study of Liver Diseases (AASLD), it is recommended that all persons with active HCV infection be linked to a healthcare provider with the knowledge and resources necessary to provide comprehensive management.28 In patients with advanced fibrosis or cirrhosis, subspecialty care may be required, especially for those eligible for consideration for liver transplantation because of hepatic decompensation. To address the lack of specialists available for patients with HCV, primary care practitioners are encouraged to collaborate via telemedicine and knowledge networks to enhance quality of care.28
Pretreatment Evaluation
Because of the asymptomatic nature of initial HCV infection, pretreatment evaluation should be initiated through screening for risk factors as mentioned previously (see Table 1).17, 18, 26, 29, 30 Although all the risk factors listed are important to evaluate for in the primary care setting, history of IDU remains the leading cause of HCV.30 The development of a patient activation toolkit can serve as an excellent resource for primary care physicians to screen individuals. However, it is important to avoid using stigmatizing language and emphasize HCV infection as inclusive to any adult.29
Table 1. Hepatitis C Virus Risk Factors17,18,26,29,30 |
|
After active HCV infection has been confirmed for a patient, attention can be directed toward selecting the proper treatment regimen (see Figure 2). Appropriate pretreatment workup and referral to a specialist, if necessary, should by initiated.31 Their pretreatment laboratory evaluation should include a complete blood count (CBC), serum albumin, albumin, bilirubin, ALT, aspartate aminotransferase (AST), creatinine, HIV antibody/antigen testing, HCV-RNA viral load, hepatitis B virus (HBV) surface antigen, and HBV core antibody. To evaluate for previous infection or immunity, hepatitis A virus (HAV) antibody and HBV surface antibody also may be considered.
Figure 2. Approach to Initiation of Antiviral Therapy Treatment Regimens32,33 |
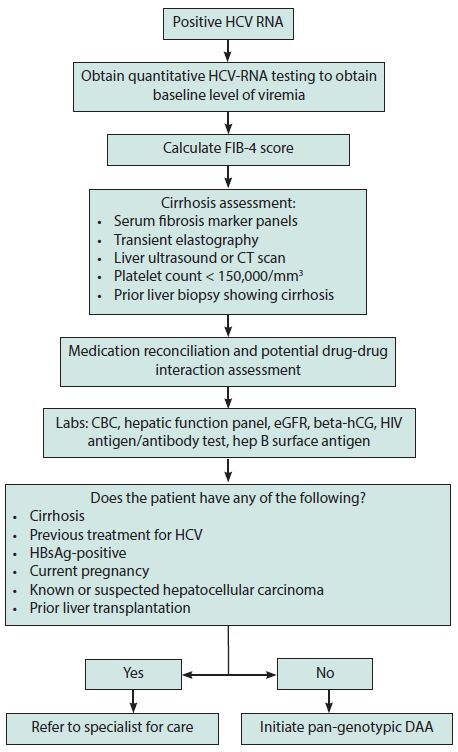 |
HCV: hepatitis C virus; RNA: ribonucleic acid; FIB-4: Fibrosis-4; CT: computed tomography; CBC: complete blood count; eGFR: estimated glomerular filtration rate; hCG: human chorionic gonadotropin; HIV: human immunodeficiency virus; HBsAg: hepatitis B surface antigen; DAA: direct-acting antiviral |
The presence of cirrhosis needs to be assessed. This can be performed by calculating a fibrosis index based on the four-factor Fibrosis-4 (FIB-4) score based on liver enzymes and platelet count. An FIB-4 score > 3.25, defines cirrhosis for the purposes of treatment. Assessment of cirrhosis, especially in patients with indeterminate FIB-4 score (1.45 to 3.25) can be assessed by using ultrasound or FibroScan-based transient elastography, serologic markers (e.g., FibroSure, Enhanced Liver Fibrosis test), clinical evidence of cirrhosis (platelet count < 100,000/mm3, liver imaging such as ultrasound or computed tomography scan demonstrating nodularity or splenomegaly), or liver biopsy showing cirrhosis.32,33 Patients then should undergo a thorough medication reconciliation. Tools such as the HEP Drug Interactions project (https://www.hep-druginteractions.org/checker) by the University of Liverpool are readily available to assess for potential drug interactions of patients’ current medication list with HCV therapies. This in turn can help determine the choice of HCV therapy that is best suited for the patient.
Next, the patient should be educated on how to administer their medications, provided with tools for proper adherence, and counseled on reinfection prevention.32
The patient also should undergo HCV genotype evaluation if required by insurance or needed for specific direct-acting antiviral (DAA) drugs. However, treatment with pan-genotypic DAA drugs does not require testing.27,32 It has been advised that patients receive quantitative HCV-RNA testing prior to initiation of antiviral therapy to obtain a baseline viral load level.32 Patients also should be advised to receive vaccination for hepatitis A and B if they have not done so already.34 However, therapy should not be delayed because of immunizations.
Along with this initial workup, to improve follow-up and ultimately achieve SVR, additional actions should be taken by primary care providers to connect patients with resources that can assist them with mental health, transportation, medication costs and delivery, and connection to treatment for substance use disorder, if applicable.34
Special Consideration for HBV Coinfection or Positive HBV Serologies
Patients meeting criteria for HBV treatment should be initiated or continued with HBV therapy. According to AASLD 2018 guidelines, HBV treatment should be offered to all patients with decompensated or compensated cirrhosis. In patients without cirrhosis, treatment should be offered if ALT is more than twice the upper limit of normal and the patient has an elevated viral load (HBV DNA > 2,000 IU/mL if HBV e antigen-negative and HBV DNA > 20,000 IU/mL if HBV e antigen-positive).35
Patients with HBV surface antigen positivity who do not meet the treatment criteria remain at risk of reactivation of HBV with HCV therapy. In these patients, prophylactic HBV therapy can be initiated and continued until 12 weeks after completion of HCV therapy. Alternatively, in patients who are averse to medical therapy and are able to follow up regularly, an HBV DNA monitoring strategy may be employed. HBV DNA levels can be monitored every month during and immediately after HCV therapy. If HBV DNA rises to more than 1,000 IU/mL or to more than 10-fold above baseline, HBV prophylactic therapy can be employed.36
Treatment Regimens
The objective of HCV treatment is to target specific processes in the HCV replication cycle to block replication and induce clearance through cell death.23 The AASLD and Infectious Diseases Society of America provide their recommended approach to HCV treatment (see Figure 3).33,37-41 Treatment regimens may vary based on whether patients have had treatment previously, their degree of cirrhosis, or which HCV genotype they have.
Figure 3. Treatment Selection Algorithm33,37-41 |
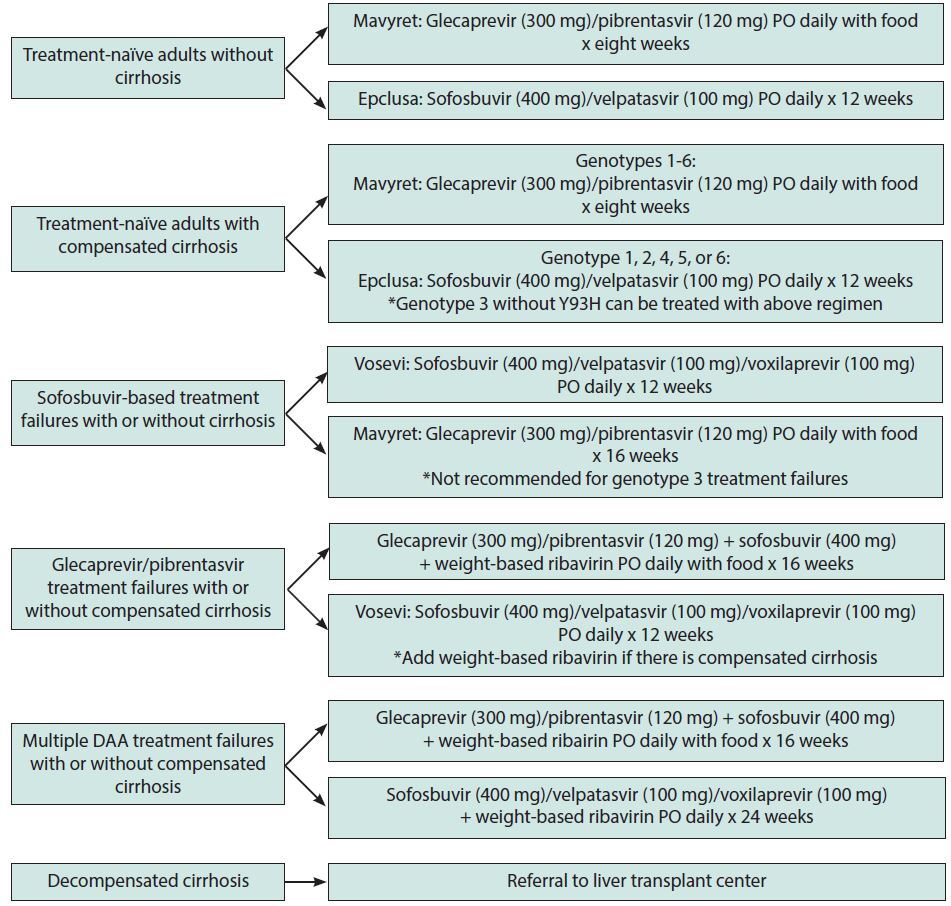
|
PO: by mouth; DAA: direct-acting antiviral |
Treatment-Naïve Adults Without Cirrhosis
If the patient has not had HCV genotype testing, they should be started on sofosbuvir (400 mg)/velpatasvir (100 mg) (brand name: Mavyret) for 12 weeks or glecaprevir (300 mg)/pibrentasvir (120 mg) (brand name: Epclusa) for eight weeks.33 These should be used in patients without cirrhosis or previous treatment for HCV.
Treatment-Naïve Adults with Compensated Cirrhosis
If the patient has never been treated for HCV but has signs of compensated cirrhosis, their treatment varies slightly. Degree of cirrhosis is evaluated using the Child-Turcotte-Pugh (CTP) classification for severity of cirrhosis calculator. Using this will determine if the patient’s cirrhosis is compensated or decompensated. The calculator uses the clinical and laboratory criteria of degree of encephalopathy, ascites, bilirubin, albumin, and international normalized ratio (INR). If their score is ≥ 7, they have decompensated cirrhosis. If their score is < 7, they have compensated cirrhosis and can follow this treatment regimen. If the genotype is unknown or is genotypes 1-6, they can be treated with glecaprevir (300 mg)/pibrentasvir (120 mg) orally daily with food for eight weeks. If they are known to have either genotype 1, 2, 4, 5, or 6, they also are eligible to be treated with sofosbuvir (400 mg)/velpatasvir (100 mg) orally daily for 12 weeks. If they have known genotype 3 HCV without the Y93H substitution, they also can be treated with Epclusa.37
Sofosbuvir-Based Treatment Failures with or Without Cirrhosis
In patients who previously have been treated for HCV infection with sofosbuvir, their treatment regimen differs independent of whether they have compensated cirrhosis. They can take sofosbuvir (400 mg)/velpatasvir (100 mg)/voxilaprevir (100 mg) (brand name: Vosevi) orally daily for 12 weeks. Another acceptable option is glecaprevir (300 mg)/pibrentasvir (120 mg) orally daily with food for 16 weeks. However, this is not recommended for genotype 3 treatment failures.38
Glecaprevir/Pibrentasvir Treatment Failures with or Without Compensated Cirrhosis
For patients who have been treated previously with Mavyret, with or without cirrhosis, their treatment regimen also is altered. They should receive glecaprevir (300 mg)/pibrentasvir (120 mg), sofosbuvir (400 mg), and weight-based ribavirin orally daily with food for 16 weeks. Alternatively, they can receive sofosbuvir (400 mg)/velpatasvir (100 mg)/voxilaprevir (100 mg) orally daily for 12 weeks. Weight-based ribavirin should be added if there is evidence of compensated cirrhosis.39
Multiple DAA Treatment Failures with or Without Compensated Cirrhosis
Additionally, in patients who have had multiple DAA treatment failures, independent of whether they have compensated cirrhosis, a longer duration of treatment is necessary. This includes treatment with glecaprevir (300 mg)/pibrentasvir (120 mg), sofosbuvir (400 mg), and weight-based ribavirin orally daily with food for 16 weeks. Instead, they also could receive sofosbuvir (400 mg)/velpatasvir (100 mg)/voxilaprevir (100 mg) with weight-based ribavirin orally daily for 24 weeks.40
Decompensated Cirrhosis
Patients with decompensated cirrhosis, defined as having a CTP score ≥ 7, have a more complicated treatment regimen. Because of their disease progression and resulting hepatic impairment, they should be referred to a liver transplant center.41
Presently, there are a few suggested regimens for HCV genotype 1 therapy. These regimens are simeprevir plus sofosbuvir with or without ribavirin; ledipasvir/sofosbuvir; and ombitasvir/paritaprevir/ritonavir plus dasabuvir, with or without ribavirin. These medications have differing effects depending on the genotype. Different combinations of paritaprevir/ritonavir/ombitasvir plus dasabuvir have been effective against genotypes 1-6, but are not as effective with genotypes 2-3. Response depends on sub-genotypic classification. Ledipasvir/sofosbuvir (brand name: Harvoni) has shown effectiveness against genotypes 1 and 4-6, but decreased effectiveness in genotypes 2-3.
Elbasvir/grazoprevir (brand name: Zepatier) with or without ribavirin has shown effectiveness against genotypes 1 and 4. Other common therapies, sofosbuvir/velpatasvir (Epclusa), glecaprevir/pibrentasvir (Mavyret), and sofosbuvir + velpatasvir + voxilaprevir (Vosevi) all have been shown to have significant effectiveness against all six genotypes.42 A summary of the average costs and duration of the most common options for HCV treatment are shown in Table 2.43
Table 2. Average Cost and Duration of Common Hepatitis C Virus Therapy43 |
|
Therapy |
Duration of Therapy and Cost* |
Epclusa (sofosbuvir/velpatasvir) |
12 weeks: $78,808 12 weeks: $24,000 (generic) |
Harvoni (ledipasvir/sofosbuvir) |
8 weeks: $65,000 12 weeks: $98,500 24 weeks: $197,000 28 tablets: $10,090 (generic) |
Zepatier |
28 tablets: $7,675 |
Vosevi |
4 weeks: $26,026 8 weeks: $52,052 12 weeks: $78,078 |
Mavyret |
4 weeks: $13,200 8 weeks: $26,400 |
* Without insurance or manufacturer assistance programs |
|
Treatment Monitoring
Treatment monitoring in patients diagnosed with HCV depends largely on each patient’s response to antiviral therapy. Patients ultimately can be divided into two groups: those who have achieved SVR and those who have not. SVR is defined as undetectable RNA 12 weeks after the completion of antiviral therapy. With this definition in mind, obtaining an HCV quantitative, full-time PCR (HCV RNA quant) at the 12-week post-therapy mark is recommended. Although not on official recommendations, some clinicians have been observed to monitor an HCV RNA quant at 24 weeks in select, high-risk populations, such as those with liver cirrhosis. Achieving SVR with the use of DAA therapy, specifically in patients who are adherent, immunocompetent, treatment-naïve, and without decompensated liver disease, exceeds 95%.
Patients who achieve SVR can be categorized further into four subgroups: those without liver cirrhosis, those with liver cirrhosis, those with persistently elevated liver enzymes, and those with ongoing risk of HCV infection. In patients without liver cirrhosis, special monitoring is not recommended. Data show that patients who achieve SVR following hepatitis C treatment do not tend to progress to HCV-related liver fibrosis; thus, they can be followed as if they were never infected with HCV.44 It should be emphasized to these patients that they are not immune to HCV and can become reinfected.
Those who achieve SVR but have received a diagnosis of cirrhosis do have follow-up recommendations, given their increased risk for development of HCC. These patients will require abdominal ultrasound (US) with or without alfa-fetoprotein (AFP) blood testing every six months, since it is standard for HCC screening. Additionally, it is recommended cirrhotic patients undergo surveillance endoscopy every two years if they are known to have small varices. In the absence of varices, endoscopy should be performed every three years, as per the AASLD.45
Patients with persistently elevated liver enzymes, such as ALT, should undergo further evaluation for other causes of liver disease, such as alcohol-associated liver disease, non-alcoholic fatty liver disease (NAFLD) or metabolic-associated fatty liver disease (MAFLD), iron overload, etc.
Those with ongoing risk of HCV reinfection should be monitored periodically for reinfection, as well as receive ongoing counseling for risk reduction. Those at risk for reinfection do not differ from those at increased risk of infection (IDU, men who have condomless sex with men, etc.). Recurrence was found to be around 1% in low-risk HCV mono-infected patients, 11% in high-risk HCV mono-infected patients (aforementioned patients), and 15% in HIV/HCV-coinfected patients. Antibody testing is not recommended for screening in this population since they likely will remain antibody-positive from their previous infection and should be tested for recurrence with HCV RNA quant. Any elevation in aminotransferase levels should warrant evaluation for reinfection as well.
In patients who achieve SVR, an important concept to consider is liver harm reduction. These patients, especially those with liver cirrhosis, should be counseled on the liver damage they already have sustained and things that may exacerbate that liver injury. Alcohol use and weight gain are two common causes of continued liver damage. This also is true in HCV-infected persons.
Beyond DAA therapy, addressing psychosocial behaviors (such as continued drug use), preventing comorbidity (such as obesity, as discussed earlier), preventing coinfections, and being immunized are mainstays. This also will become vital for these patients when they do achieve SVR, since many of the aforementioned behaviors are associated with reinfection.
It is important to identify reinfection promptly, since this, in conjunction with treatment, can prevent transmission and complications. The HERO study found that reinfection was associated with younger age at diagnosis and methamphetamine detection.46 Other associated risks included needle sharing, spousal use of injection drugs, housing instability, and incarceration.47
Those patients who do not achieve SVR and are not undergoing retreatment, or who have failed a second/third DAA treatment course, will have several screening labs drawn every six to 12 months, including a hepatic function panel, CBC, and INR to monitor for liver inflammation and evaluate function. On top of these screenings, patients should be encouraged to abstain from alcohol and avoid hepatotoxic medications, such as acetaminophen. Patients who qualify under this distinction and have developed liver cirrhosis should undergo the same screening for HCC as those patients discussed previously (abdominal US, possible serum AFP, baseline upper endoscopy).
Other considerations for treatment monitoring are clinic or telehealth follow-up to assess medication adherence and for possible side effects or drug-drug interactions. Patients taking diabetic medications are at increased risk of symptomatic hypoglycemia and should be closely monitored. Patients taking warfarin may experience changes to their anticoagulation status, and close INR monitoring is advised. Patients taking elbasvir/grazoprevir therapy should complete a hepatic function panel at eight and 12 weeks if they are receiving the 16-week course. If a patient undergoing DAA therapy experiences a 10-fold increase in ALT, therapy should be discontinued. If an increase in ALT by less than 10-fold is seen, those experiencing liver inflammation or increased conjugated bilirubin, ALP, or INR should discontinue DAA therapy. Asymptomatic increases in ALT less than 10-fold should have biweekly monitoring. Patients with persistent elevation should be considered for discontinuation.
Patients who do not achieve SVR remain at risk for worsening liver injury and progression of hepatic fibrosis. They also carry the potential to transmit the virus to others and should be considered for retreatment. It is possible that these patients carry a virus that is resistant to one or more antivirals.45 Uncertainty surrounding resistance and resistance testing warrants expert consultation.
HCV can be treated by a patient’s primary care physician; in fact, the CDC encourages family physicians to treat hepatitis C.48 When primary care physicians prescribe DAA, specifically to patients with uncomplicated hepatitis C, outcomes are comparable to those seen with subspecialists.48 Primary care health professionals are the first line of medical practitioners. This group is instrumental in screening for and treating hepatitis C. Simplified care delivery could be best for this patient population. Obtaining screening, genotyping, and diagnosis, as well as treatment, all from one practitioner can help to centralize care, therefore increasing rates of screening and treatment. This can be done more efficiently with access to point-of-care RNA testing as well as information on treatment options and best practices. Other essential settings include sexual health clinics, substance use clinics, and community health centers.
Those patients with complicated cases or who develop cirrhosis of the liver should be referred to subspecialists.49 Other special populations, including those on immunosuppressive therapy or chemoradiation, or pregnant patients, do have special considerations but do not require specialty consultation. There is no evidence to suggest reactivation is more common in patients on immunosuppressive therapy or chemoradiation; therefore, more frequent monitoring than others who have achieved SVR is not recommended. Women of childbearing potential should not receive ribavirin in the six months prior to pregnancy and should be counseled not to become pregnant while receiving a regimen including ribavirin.45 Additionally, male partners of women of childbearing potential should receive the same cautions. Serum pregnancy testing in these populations is recommended prior to starting this medication.
Challenges and Future Direction in the Eradication of HCV
HCV eradication has emerged as a critical goal in public health because of its likelihood to result in chronic infection, leading to numerous complications. It has placed a significant burden of disease on the American healthcare system; in 2011, Medicare spent more than $6.5 billion on HCV infection, with the total cost expected to rise to $9.1 billion in 2024.50 Aside from the financial burden HCV places on the American healthcare system, HCV infection can lead to significant personal health concerns, both physiological and psychological, making eradication of HCV a top priority of many top governmental agencies in the world.
The White House has proposed a national initiative for HCV eradication for 2024. The White House’s plan has, essentially, four key aspects: identification of more cases through expansion of access to single visit rapid-result testing, expansion of access to care for Medicaid users via elimination of existing requirements, reduction of cost for screening and treatment through negotiations with pharmaceutical companies for a subscription model for therapies, further investing in community programs for care, and development of HCV vaccination. To obtain these visions put forth by the White House, a 2024 budget proposal was submitted to Congress to set aside $12.3 billion over the next 10 years to eliminate HCV.
From page 79 of the proposed budget: “The Budget includes a new mandatory proposal for a national program to significantly expand screening, testing, treatment, prevention, and monitoring of hepatitis C infections in the United States, with a specific focus on populations with high infection levels. This program would support Federal procurement of life-saving treatments, while bolstering provider capacity and related public health efforts such as testing, communication, and surveillance.”
However, eradication of a disease is not an easy task; to date, only one disease has faced total eradication (smallpox, with another, polio, close behind). Despite significant advances in technology, updated testing guidelines, and treatment modalities, several challenges persist precluding the goal of global HCV eradication. HCV has been appropriately labeled a “silent epidemic” because of the natural course of the disease. HCV smolders internally — silently — taking its toll on the infected individual over a prolonged period and generally does not have the visible debilitation associated with other diseases (e.g., smallpox and polio).
The prolonged latent period of HCV and lack of visible debilitations continues to lead to one of the most significant challenges, infection identification. Of the nearly 200 million privately insured Americans, 1.5%, or 3 million, of them were found to have HCV, with roughly 87%, or about 588,818, going undiagnosed.51 This incredible proportion of undiagnosed individuals hinders efforts to initiate treatment in a timely manner, preventing disease progression as well as stifling unknowing transmission. Outreach programs, community-based testing, and increased awareness of HCV, as well as updated screening guidelines among the healthcare community, are crucial components in addressing this challenge.
Further recommendations include universal screening for everyone at least once, but specific targeting and repeat screening of high-risk individuals, such as incarcerated people, IV drug users, men who have sex with men, persons who are HIV-positive, and homeless persons. The first step in the eradication of HCV is identification of the undiagnosed population so they can be treated effectively, and to prevent disease progression and further transmission. The use of the electronic medical record (EMR) is a relatively untapped resource in the identification of undiagnosed HCV. There are multiple capabilities of EMR that could help with identification, such as alerts, order sets, data collection/sharing, and tracking. Additionally, establishing a Healthcare Effectiveness Data and Information Set (HEDIS) measure for HCV would provide incentive for healthcare systems to achieve identification, management, and treatment for HCV.52
Furthermore, telemedicine is a resource and technology that can be used to better identify these individuals and has the ability to overcome barriers to treatment, such as temporal and geographical obstacles. A study regarding the use of telemedicine in the identification and treatment of patients with HCV was conducted by Talal et al. A model of facilitated telemedicine was used and focused on opioid treatment programs as a recruiting center; this is because people with opioid addiction tend to have a higher risk of HCV incidence and prevalence.53 All patients at the opioid treatment center were screened for HCV, evaluated by a provider via telemedicine, and received HCV medications dispensed with the patients’ existing methadone dose. Talal et al found sustained virological response (SVR; undetectable HCV RNA three months post-treatment completion) was substantially higher in facilitated telemedicine (90.7%) compared to referral (35.2%). Project ECHO from the University of California San Francisco (UCSF) is another program looking to combat HCV via telemedicine. Project ECHO is a knowledge-sharing network created to help providers care for patients with HCV in community centers.
An additional barrier to eradication is the accessibility of obtaining DAA therapy. Since the introduction of DAA, the HCV treatment landscape has been revolutionized substantially through high cure rates and short treatment durations compared to traditional interferon-based regimens. Even more promising is the potential for a one-time injection treatment rather than a treatment with a high pill burden for a prolonged period of time. It has been found that glecaprevir-pibrentasvir one-time intramuscular (IM) injection has a higher trough than an eight-week oral course, showing promise for a one-time injection treatment.53 A one-time injection treatment would dramatically reduce treatment failure caused by lack of follow-up and/or noncompliance. However, like most new medications marketed for chronic illness, there is a substantial cost associated with obtaining these medications.
Although it has been noted that HCV treatment is becoming more cost effective, many U.S.-based insurers are continuing to limit access to HCV treatment.54 This limited access is a result of the high cost of HCV medication as well as the substantial prevalence of the disease. However, compared to previous years, it is in fact becoming more affordable, but with continued talks of budgetary cuts to Medicaid, there likely will be further limitations to HCV treatment in the future. This only takes into account the insured, but some promise lies ahead with the proposed White House budget for 2024 as mentioned previously.
Lastly, the issue of reinfection remains a concern, particularly among high-risk populations such as IV drug users. Comprehensive harm reduction strategies, including needle exchange programs, addiction treatment services, and education, are integral to addressing the risk of reinfection. Multidisciplinary approaches that involve the healthcare community as a whole, and community organizations, are essential to create a supportive environment for individuals at risk of HCV reinfection.55
Conclusion
There are many barriers to the eradication of HCV, from infection identification to treatment, making it a very complex public health concern. Unfortunately, no vaccine for HCV exists yet, and development proves difficult because of the overwhelming genetic diversity. Thus, we must rely on the strategies discussed previously until our technology progresses to a point where a vaccine is widely available, with adequate longitudinal data depicting its safety and efficacy for the treatment and prevention of HCV.
References
- Centers for Disease Control and Prevention. 2020 viral hepatitis surveillance report. Last reviewed Aug. 18, 2022. https://www.cdc.gov/hepatitis/statistics/2020surveillance/index.htm
- Centers for Disease Control and Prevention. What is viral hepatitis? Last reviewed Oct. 2, 2023. https://www.cdc.gov/hepatitis/abc/index.htm
- World Health Organization. Hepatitis C. July 18, 2023. https://www.who.int/news-room/fact-sheets/detail/hepatitis-c
- El-Serag HB, Rudolph KL. Hepato-cellular carcinoma: Epidemiology and molecular carcinogenesis. Gastroenterology 2007;132:2557-2576.
- Martinez MA, Franco S. Therapy implications of hepatitis C virus genetic diversity. Viruses 2020;13:41.
- Echeverría N, Comas V, Aldunate F, et al. In the era of rapid mRNA-based vaccines: Why is there no effective hepatitis C virus vaccine yet? World J Hepatol 2021;13:1234-1268.
- Henry B. Drug pricing & challenges to hepatitis C treatment access. J Health Biomed Law 2018;14:265-283.
- Faccioli J, Nardelli S, Gioia S, et al. Neurological and psychiatric effects of hepatitis C virus infection. World J Gastroenterol 2021;27:4846-4861.
- Brunner N, Bruggmann P. Trends of the global hepatitis C disease burden: Strategies to achieve elimination. J Prev Med Public Health 2021;54:251-258.
- Williams I. Epidemiology of hepatitis C in the United States. Am J Med 1999;107:2S-9S.
- Stasi C, Silvestri C, Voller F. Update on hepatitis C epidemiology: Unaware and untreated infected population could be the key to elimination. SN Compr Clin Med 2020;2:2808-2815.
- Centers for Disease Control and Prevention. Hepatitis C: By the numbers. CDC Fact Sheet. https://www.cdc.gov/nchhstp/newsroom/docs/factsheets/Hepatitis-c-by-the-numbers.pdf
- Hepatitis C Online. Lesson 2. Recommendations for hepatitis C screening. https://www.hepatitisc.uw.edu/go/screening-diagnosis/recommendations-screening
- Centers for Disease Control and Prevention. Sexual transmission and viral hepatitis. Last reviewed Sept. 21, 2020. https://www.cdc.gov/hepatitis/populations/stds.htm
- Axley P, Ahmed Z, Ravi S, Singal AK. Hepatitis C virus and hepatocellular carcinoma: A narrative review. J Clin Transl Hepatol 2018;6:79-84.
- Russo FP, Zanetto A, Pinto E, et al. Hepatocellular carcinoma in chronic viral hepatitis: Where do we stand? Int J Mol Sci 2022;23:500.
- Centers for Disease Control and Prevention. Testing recommendations for hepatitis C virus infection. Last reviewed Oct. 31, 2023. https://www.cdc.gov/hepatitis/hcv/guidelinesc.htm
- Schillie S, Wester C, Osborne M, et al. CDC recommendations for hepatitis C screening among adults – United States, 2020. MMWR Recomm Rep 2020;69:1-17.
- Centers for Disease Control and Prevention. Test for hepatitis C during every pregnancy. Last reviewed May 27, 2021. https://www.cdc.gov/knowmorehepatitis/hcp/Test-For-HepC-During-Pregnancy.htm
- Zein NN. Clinical significance of hepatitis C virus genotypes. Clin Microbiol Rev 2000;13:223-235.
- U.S. Department of Veterans Affairs. Viral hepatitis and liver disease. Genotypes: Hepatitis C. Last updated Oct. 23, 2018. https://www.hepatitis.va.gov/hcv/background/genotypes.asp
- Fourati S, Feld JJ, Chevaliez S, Luhmann N. Approaches for simplified HCV diagnostic algorithms. J Int AIDS Soc 2018;21 Suppl 2(Suppl Suppl 2):e25058.
- Parsons G. Hepatitis C: Diagnosis, treatment and harm-reduction strategies. Prescriber 2022;33:23-28.
- Keikha M, Eslami M, Yousefi B, et al. HCV genotypes and their determinative role in hepatitis C treatment. Virusdisease 2020;31:235-240.
- Rabaan AA, Al-Ahmed SH, Bazzi AM, et al. Overview of hepatitis C infection, molecular biology, and new treatment. J Infect Public Health 2020;13:773-783.
- Dermont M, Sullivan R, Sibal B, et al. Hepatitis C diagnosis and management: A primary care and public health partnership approach. Br J Gen Pract 2022;72:89-92.
- Wang AE, Hsieh E, Turner BJ, Terrault N. Integrating management of hepatitis C infection into primary care: The key to hepatitis C elimination efforts. J Gen Intern Med 2022;37:3435-3443.
- Center for Health Law and Policy Innovation. Hepatitis C: The state of Medicaid access: May 2021 national progress report. Published May 19, 2021. https://stateofhepc.org/wp-content/uploads/2021/06/HCV_State-of-Medicaid-Access_May-2021-Progress-Report.pdf
- Rivera Rivera J, Fuzzell LN, Garcia J, et al. Development of a patient activation toolkit for hepatitis C virus testing. J Cancer Educ 2023;38:931-939.
- Dimova RB, Rude E, Talal AH. Age- and risk factor-based serologic screening for hepatitis C virus among an urban, high-risk population. J Viral Hepat 2020;27:1369-1387.
- Marukutira T, Barter R, Moore KP, et al. Connecting patients notified with hepatitis C to treatment (CONNECT Study): A randomized controlled trial of active case management by a health department to support primary care practitioners. Int J Drug Policy 2023;121:104184.
- American Association for the Study of Liver Diseases, Infectious Diseases Society of America. HCV testing and linkage to care. Last updated Oct. 24, 2022. https://www.hcvguidelines.org/evaluate/testing-and-linkage
- American Association for the Study of Liver Diseases, Infectious Diseases Society of America. Simplified HCV treatment for treatment-naïve adults without cirrhosis. Last updated Dec. 19, 2023. https://www.hcvguidelines.org/treatment-naive/simplified-treatment
- Stewart A, Craig-Neil A, Hodwitz K, et al. Increasing treatment rates for hepatitis C in primary care. J Am Board Fam Med 2023;36:591-602.
- Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018;67:1560-1599.
- Bhattacharya D, Aronsohn A, Price J, Lo Re V; AASLD-IDSA HCV Guidance Panel. Hepatitis C guidance 2023 update: AASLD-IDSA recommendations for testing, managing, and treating hepatitis C virus infection. Clin Infect Dis 2023; May 25:ciad319. doi: 10.1093/cid/ciad319. [Online ahead of print].
- American Association for the Study of Liver Diseases, Infectious Diseases Society of America. Simplified HCV treatment for treatment-naïve adults with compensated cirrhosis. Last updated Dec. 19, 2023. https://www.hcvguidelines.org/treatment-naive/simplified-treatment-compensated-cirrhosis
- American Association for the Study of Liver Diseases, Infectious Diseases Society of America. Sofosbuvir-based and elbasvir/grazoprevir treatment failures. Last updated Oct. 24, 2022. https://www.hcvguidelines.org/treatment-experienced/sof-and-elb-grz-failures
- American Association for the Study of Liver Diseases, Infectious Diseases Society of America. Glecaprevir/pibrentasvir treatment failures. Last updated Oct. 24, 2022. https://www.hcvguidelines.org/treatment-experienced/g-p-failures
- American Association for the Study of Liver Diseases, Infectious Diseases Society of America. Multiple DAA treatment failures (all genotypes), including sofosbuvir/velpatasvir/voxilaprevir or sofosbuvir plus glecaprevir/pibrentasvir. Last updated Oct. 24, 2022. https://www.hcvguidelines.org/treatment-experienced/multiple-daa-failure
- American Association for the Study of Liver Diseases, Infectious Diseases Society of America. Patients with decompensated cirrhosis. Last updated Oct. 24, 2022. https://www.hcvguidelines.org/unique-populations/decompensated-cirrhosis
- Geddawy A, Ibrahim YF, Elbahie NM, Ibrahim MA. Direct acting anti-hepatitis C virus drugs: Clinical pharmacology and future direction. J Transl Int Med 2017;5:8-17.
- Drugs.com. https://www.drugs.com/drug_information.html
- Corcorran MA, Kim N. Monitoring during and after HCV treatment. Hepatitis C Online. Last updated Oct. 5, 2023. https://www.hepatitisc.uw.edu/go/treatment-infection/monitoring/core-concept/all#:~:text=Patients%20should%20have%20a%20quantitative,cure%20for%20nearly%20all%20patient
- American Association for the Study of Liver Diseases, Infectious Diseases Society of America. Monitoring patients who are starting HCV treatment, are on treatment, or have completed therapy. Last updated Dec. 19, 2023. https://www.hcvguidelines.org/evaluate/monitoring
- Litwin AH, Jost J, Wagner K, et al; HERO Study Group. Rationale and design of a randomized pragmatic trial of patient-centered models of hepatitis C treatment for people who inject drugs: The HERO study. Contemp Clin Trials 2019;87:105859.
- Kim AY. Life after hepatitis C cure: Reinfection, harm reduction, and long-term monitoring for liver complications. Presented at the American Association for the Study of Liver Diseases: The Liver Meeting. Boston; Nov. 10, 2023.
- Andrews RR. Family physicians can manage adults with hepatitis C. American Family Physician. Published Oct. 1, 2018. https://www.aafp.org/pubs/afp/issues/2018/1001/p413.html
- Martinez A. Meeting patients where they are: What is the role of the hepatitis C specialist in community-based hepatitis C care? Presented at the American Association for the Study of Liver Diseases: The Liver Meeting. Boston; Nov. 10, 2023.
- Hagan LM, Schinazi RF. Best strategies for global HCV eradication. Liver Int 2013;33 Suppl 1(0 1):68-79.
- Razavi H, Elkhoury AC, Elbasha E, et al. Chronic hepatitis C virus (HCV) disease burden and cost in the United States. Hepatology 2013;57:2164-2170.
- Talal A. Facilitated telemedicine for underserved populations: A stepped wedge trial of hepatitis C treatment. Presented at the American Association for the Study of Liver Diseases: The Liver Meeting. Boston; Nov. 10, 2023.
- Thomas D. New innovations to eliminate hepatitis C. Presented at the American Association for the Study of Liver Diseases: The Liver Meeting. Boston; Nov. 10, 2023.
- American Association for the Study of Liver Diseases, Infectious Diseases Society of America. Overview of cost, reimbursement, and cost-effectiveness considerations for hepatitis C treatment regimens. Last updated Oct. 24, 2022. https://www.hcvguidelines.org/evaluate/cost
- Fox RK. Implementing health systems solutions: Harnessing the EMR to improve hepatitis C screening, linkage, and treatment. Presented at the American Association for the Study of Liver Diseases: The Liver Meeting. Boston; Nov. 10, 2023.
Hepatitis C accounts for a significant burden of disease. There are many barriers to the eradication of hepatitis C virus (HCV), from infection identification to treatment, making it a very complex public health concern. Unfortunately, no vaccine for HCV exists yet, and development proves difficult because of the overwhelming genetic diversity. HCV can be treated by a patient’s primary care physician; this group is instrumental in screening for and treating hepatitis C.
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.