The featured electrocardiogram (ECG) was obtained following successful resuscitation from cardiac arrest. Although echo done soon after showed akinesis of the anterior wall, no significant coronary narrowing was seen on cardiac catheterization. Can you explain? What is this phenomenon called?
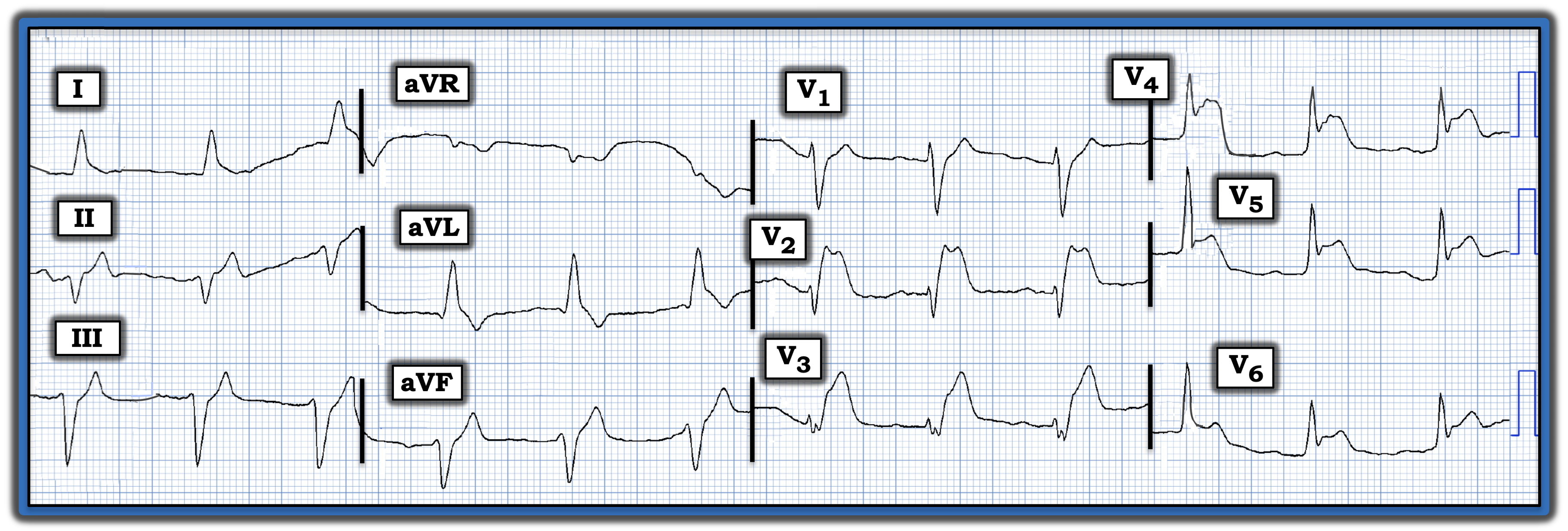
Interpretation: From today’s ECG, one would expect to see on cardiac catheterization clear evidence of acute proximal left anterior descending coronary artery occlusion, especially in view of the anterior wall motion abnormality seen on echo.
- • The rhythm in this ECG is supraventricular, given the narrow QRS complexes. Although P waves are not well seen in lead II, small-but-present P waves with a fixed PR interval are seen in leads V1 and V2.
- • There is marked left axis deviation and a prominent Q wave in lead aVL. But the most remarkable findings are the loss of anterior R wave forces, fragmentation of the QRS in lead V3 — and marked ST elevation beginning in lead V2 and extending until lead V6.
The ECG findings raise the question of how to explain the absence of a “culprit” artery on cardiac catheterization performed soon after successful resuscitation from cardiac arrest.
- Many clinicians are not aware of the entity known as “MINOCA” (myocardial infarction with non-obstructive coronary arteries). Although the term MINOCA was adopted in 2013, the concept that myocardial infarction may occur despite patent coronary arteries had been described decades earlier.
- The three most common causes of an acute coronary syndrome despite normal coronary anatomy are acute myocarditis, Takotsubo cardiomyopathy, and MINOCA.
- Although a number of entities have been associated with MINOCA (including coronary artery vasospasm, severe anemia, arrhythmias, valvular disease, and acute respiratory failure), the most common cause of MINOCA appears to be acute infarction from coronary occlusion, in which the “culprit” artery spontaneously reperfuses, such that no significant coronary stenosis is visible by the time cardiac catheterization is done. Given the ECG appearance of today’s tracing, spontaneous reperfusion of acute coronary occlusion was deemed the most likely explanation for the negative cardiac catheterization result.
- All clinicians involved in emergency care will encounter MINOCA — this entity is estimated to occur in as many as 10% of patients who initially are diagnosed as having acute myocardial infarction.
The featured electrocardiogram was obtained following successful resuscitation from cardiac arrest. Although echo done soon after showed akinesis of the anterior wall, no significant coronary narrowing was seen on cardiac catheterization. Can you explain? What is this phenomenon called?
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.