By Ken Grauer, MD
Professor Emeritus in Family Medicine, College of Medicine, University of Florida
The ECG in the figure below is from an older man who presented with an acute stroke. He denied chest pain. Why is there QRS widening? What might be the clinical implications?
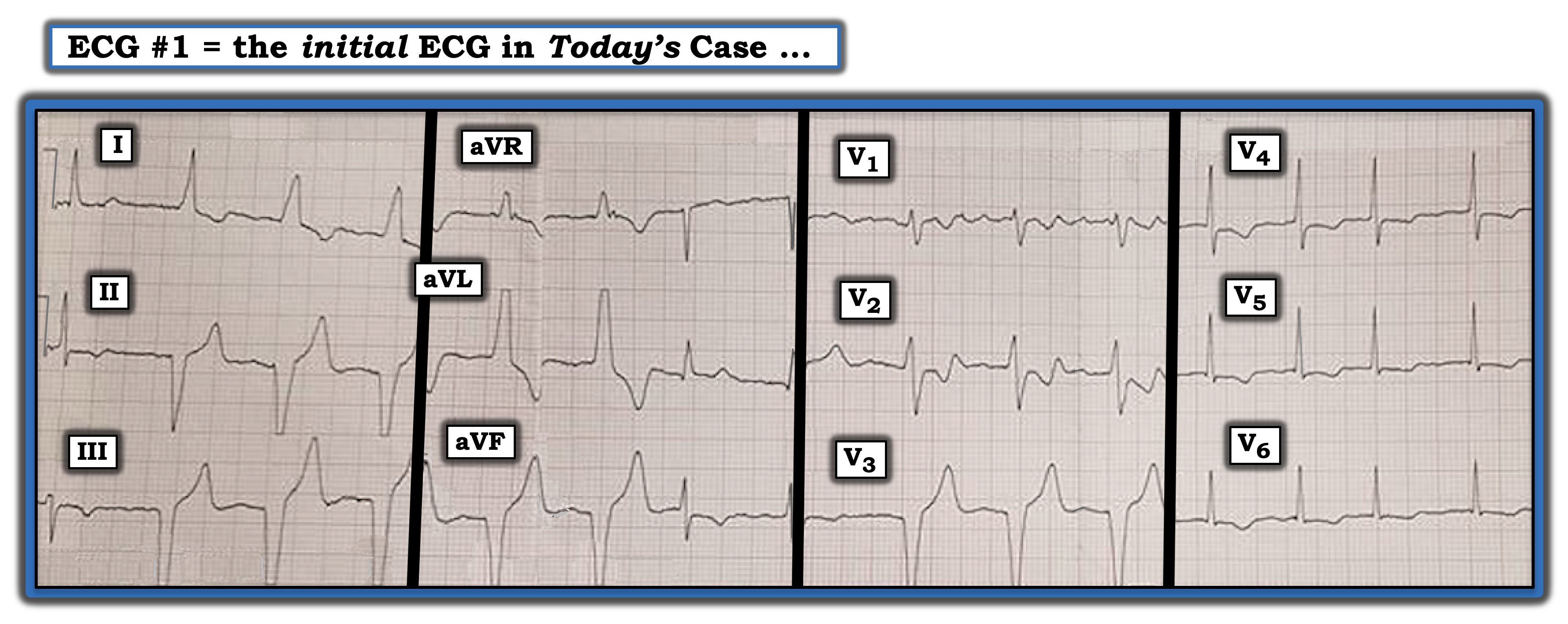
Three features complicate interpretation of this tracing: QRS morphology is changing throughout the ECG, there is no long lead rhythm strip, and QRS amplitude is “cut off” in multiple leads such that we simply do not know the size of many QRS complexes. The first beat in the tracing is narrow. This is followed by five consecutive wide beats; then two narrow beats (the second of which is partially hidden by the lead change); three wide beats in leads V1, V2, and V3; and then four narrow beats in leads V4, V5, and V6 to complete the tracing.
The key is to assess the underlying rhythm. Our best hint of this underlying rhythm is from the last four beats in the ECG, which are narrow, irregular, and without sign of atrial activity. This suggests the underlying rhythm is atrial fibrillation with a controlled ventricular response. No P waves are visible anywhere. However, the eight wide beats on this ECG manifest a surprisingly consistent R-R interval. This strongly suggests the underlying atrial fibrillation rhythm is interrupted by an accelerated idioventricular rhythm (AIVR) at ~85 beats per minute. There remains the question of ST-T wave changes. These are best assessed in this tracing by looking at the supraventricular (narrow QRS) complexes in each of the 12 leads. Doing so suggests there is moderate T wave inversion in each of the three inferior leads (II, III, and aVF) and shallow T wave inversion with ST depression in the lateral chest leads (V4, V5, and V6).
We learn this tracing was taken from an elderly man who presented with an acute stroke. His underlying atrial fibrillation predisposed him to experiencing an acute cardiovascular event. An acute myocardial infarction (MI) is the cause of a stroke in a small but significant percentage of patients. On occasion, the first ECG sign of an acute MI may be the presence of AIVR, which is a common “reperfusion” arrhythmia. It will be important to assess this patient for the possibility of a recent or acute MI.
For more information about and further discussion of this case, please visit here.
The ECG in the figure is from an older man who presented with an acute stroke. He denied chest pain. Why is there QRS widening? What might be the clinical implications?
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.