EXECUTIVE SUMMARY
Gun violence is a leading cause of death in the United States, with 45,000 deaths annually, and is the leading cause of death for children younger than 19 years of age.
- Primary care physicians are uniquely positioned to provide counseling and other interventions to effectively identify those at heightened risk.
- Although political pressures, privacy issues, and discomfort with the topic may lead some clinicians to avoid conversations with their patients about guns and the effect of gun violence, the magnitude and repercussions of gun violence make it a public health priority.
- To begin a conversation with patients about firearm safety, every medical provider should be aware of the general principles of safe storage of firearms in the home (and be open to individualization, depending on firearm use): to store guns secured/locked and unloaded and to keep ammunition secured/locked and separate from the firearms.
- There are no state or national laws or regulations that prohibit conversations with patients about firearms. Multiple studies have confirmed that patients generally are receptive to such discussions, especially if there is an awareness that someone in the household is at risk.
- People aged 85 years and older have the highest rate of suicide, followed by those aged 75 to 84 years. Suicide is the 11th leading cause of death in the United States. Although only 5% of attempts are via firearms, more than half of completed suicides are via firearms.
- Consider risk factors (including age, cognitive status, substance misuse history, and availability of firearms) when working with patients who own guns and consider harm-reducing interventions.
Fighting back tears, the usually composed 62-year-old grandfather of 14-year-old Micha says, “I don’t know what I was thinking — I will never forgive myself for leaving out those guns.”
Micha, struggling with anxiety and receiving treatment for depression, had left school abruptly and used her key to enter her nearby grandparents’ house, where she discovered three firearms on the table and bullets nearby. Her grandfather later explained, “I was cleaning the guns, but my wife called with car trouble, so I dropped everything to go help her.” A few months later, after partially recovering from a suicide attempt with one of the firearms, Micha said, “When I saw the guns, it felt like they had the answer to my problems. I had thought about suicide before, but never with a gun until that day.”
There are too many scenarios out there like the one of Micha and her grandparents. Although the politics of gun ownership are fiercely debated in the United States, for all those like Micha and the affected families, friends, and medical professionals, the politics are far outweighed by the medical aftermath, mental health implications, and deeply devastating reverberations of intentional and unintentional gun violence.
Primary care providers (PCPs) are in a unique position to lead the way in a campaign to reduce harm from firearms. There remains an urgent need for more research to fully define the scope and limits of the role of the PCP in this area, as well as to better understand the efficacy of counseling and other interventions and how to effectively identify those at heightened risk.
Consider the following statistics:
• Gun violence is a leading cause of premature death in the United States. More than 45,000 Americans died from gun violence in 2020 (a substantial increase from previous years).1,2
• Fifty-four percent of the deaths were self-inflicted (suicide), 43% related to homicide, and the remainder were unintentional or related to a police encounter; just less than 1% were from public mass shootings.1,2
• A 2019 study found that, overall, only 8.5% of suicide attempts result in a fatality while almost 90% of suicide attempts via firearm end in death.1-3
• Guns are the leading cause of death in the United States for children younger than 19 years of age, accounting for 20% of deaths in this age group in 2020.1,4
• Black men are disproportionally affected by gun violence — 52% of gun homicide victims in the United States are from this group.1,2
• Victims of domestic violence are five times more likely to be killed if the perpetrator has access to a gun than if no such access exists.1,2
• Nearly one-third of households in the United States possess one or more firearms.1,2
The scope of the problem is such that the American Public Health Association (APHA) has identified gun violence as a public health problem and recommends a “comprehensive public health approach.”5
The prevention of violent behavior is a complex and multifaceted issue. For more than a century, researchers have studied the mechanisms driving the spread of violence and what appears to be a self-perpetuating cycle. In 1890, a French sociologist studying the aftermath of the Jack the Ripper murders remarked that “infectious epidemics spread with the air or the wind; epidemics of crime follow the line of the telegraph.” Similarly, an uptick in violent crimes was observed following the assassination of John F. Kennedy in the 1960s. During that same time period, Dr. Martin Luther King Jr. noted, “violence begets violence … It is all a descending spiral, and the end is destruction — for everyone.”6
Although the thinking at the time was that the spread of violence represented a social phenomenon, research with modern-day imaging and other tools is beginning to reveal a complex interplay between neurobiological, psychosocial, and socioeconomic factors involved in the spread of violent behavior.6,7
The concept of considering violence and the spread of violent behavior as akin to the spread of a contagious disease was proposed and further explained in a 2013 National Academy of Medicine report.8 This idea was further refined by Dr. Gary Slutkin, an epidemiologist from the University of Illinois Chicago School of Public Health, who wrote in 2018 “… violence affects the structure and function of the brain, has characteristic signs and symptoms, and causes morbidity and mortality. Violence also demonstrates the characteristics of an epidemic type of disease, specifically through its clustering, spread, and transmission.”8,9
Dr. Slutkin, drawing on his experience in the management of contagious disease outbreaks, has suggested that epidemiological techniques can be used to analyze and comprehend the diffusion of violent behavior, laying the groundwork for the formulation of evidence-based preventive measures. He and other researchers have highlighted that preventive measures in the office of the PCP often begin with discussion and education regarding access to guns and exposure to violence. Although political pressures, privacy issues, and discomfort with the topic may lead some clinicians to avoid conversations with their patients about guns and the effect of gun violence, the magnitude and repercussions of gun violence make it a public health priority.9,10
In early 2022, “Consensus-Driven Priorities for Firearm Education Among Medical Professionals” was published, representing the first national guidelines on this topic and reflecting the growing awareness of the need for education to address gun violence prevention in medical care.11 Seven categories regarding the context of firearm injury (and 51 educational priorities in total) were identified:
• General (understanding basic epidemiology, patterns, and risks);
• Patient-centered care (general clinical application);
• Intimate partner violence priorities;
• Mass violence priorities;
• Peer violence priorities;
• Suicide priorities;
• Unintentional injury priorities.
PCPs have the potential to play a key role in reducing gun violence in their communities. In the 1970s, Tennessee pediatrician Dr. Robert Sanders and his wife, Patricia, demonstrated the effect of a clinician voice and the power of preventive medicine when they took on the issue of child safety car seats. Facing opposition from those who thought that car safety was a matter of individual choice, Dr. and Mrs. Sanders lobbied the state legislature regarding the lifesaving potential of a well-designed car seat. Thanks to their efforts, the first mandatory child safety seat law was passed in Tennessee in 1977, and the state rapidly saw a significant reduction in car crash mortality among children. Other states soon followed suit, illustrating the positive effect of preventive measures.12
To begin a conversation with patients about firearm safety, every medical provider should be aware of the general principles of safe storage of firearms in the home (and be open to individualization depending on firearm use):
• Store guns secured/locked and unloaded.
• Keep ammunition secured/locked and separate from the firearms.13
To help with perspective, this paper starts with an overview of the historical role of firearms in America, followed by research regarding reduction of harm from firearms with a focus on medical evidence for the role of the PCP in this arena. The second portion of the paper includes several clinical vignettes (for illustrative purposes), a brief section on gun violence and substance misuse, and online tools for the clinician.
Historical Perspective
The United States has by far the highest rate of firearm deaths of all high-income countries, at 4.7 deaths per 100,000 people. Chile and Canada follow with 1.82 and 0.5 deaths per 100,000, respectively. In addition, the United States has an alarmingly high proportion of childhood firearm deaths compared to other nations.1,14 Not surprisingly, the United States also has the highest rate of gun ownership in the world (not just among high-income countries), at an estimated 120.5 guns per 100 residents in 2018, and likely climbing during the early years of the COVID-19 pandemic when gun purchases soared.1,14
The fascination Americans have with guns can be traced back to the nation’s formation, with various events, movements, and beliefs playing a role. Historians note that the desire to own guns and the debate around gun control dates to the Revolutionary War era and the expansion westward. Gun control, which prohibited the sale of firearms to servants, slaves, and Native Americans, emerged at the same time as gun rights and the adoption of the Second Amendment. In the 1800s, towns on the frontier started passing laws to regulate gun violence, but early federal attempts to require gun inspection and safe ammunition storage largely were ignored. It was the rise of organized crime in the early 1900s that eventually spurred more robust efforts toward enforceable federal gun control laws.15,16
The 1960s ushered in the birth of the modern-day gun rights battle in the United States. Ironically, the first restrictive gun law in California (the landmark “Mulford Act” of 1967, which repealed open carry laws) was backed by the National Rifle Association (NRA), an organization today entrenched in the “gun rights” camp. Many believe the rise of the Black Panther Party in California at the time and their use of the Second Amendment to defend the right to carry firearms, as well as the assassinations of several prominent politicians, contributed to a wave of restrictive state and federal gun laws.16,17
Within 10 years, the NRA, after a change in leadership, pivoted from backing gun control legislation to lobbying to keep government out of gun control. Additionally, in the 1980s and early 1990s, the Centers for Disease Control and Prevention (CDC) launched a series of research efforts to examine the effect of gun violence, including a study published in the New England Journal of Medicine, that found an association between keeping a gun in the home and the risk of homicide.17 Representatives from the NRA and other groups were concerned that such studies were politically motivated and began a series of efforts to curtail government-funded research on gun violence.18
The Dickey Amendment of 1996 prohibited federal agencies, such as the CDC or the National Institutes of Health (NIH), from using federal funds to “advocate or promote gun control.” Although research on gun violence was not overtly targeted, the effect was an immediate decline in firearm-related research at many levels.18 In 2018, after a series of mass shootings, the RAND Corporation (a nonprofit think tank) dedicated more than $20 million to fund nonbiased research in this field.19 In 2019, Congress addressed this issue by specifically authorizing the CDC and NIH to split $25 million yearly on gun violence research. As a result, a surge of new research is on the horizon, with efforts being made to more accurately address quantification, data collection, and prevention on multiple levels, including individual, family, neighborhood, and community.20
In the introduction to a 32-article special edition of Preventive Medicine in December 2022, South et al said, “high-quality, policy-relevant science, especially work that is rooted in the power of those most directly impacted by gun violence, can be a guidepost for us all.”21
South et al also noted the “This Is Our Lane” movement as one of the factors affirming the role of medical providers in gun violence prevention. This movement began after a derogatory tweet (“someone should tell self-important anti-gun doctors to stay in their lane”) from the NRA following the release of a position paper from the American College of Physicians on reducing firearm injuries and death. Many healthcare providers responded with the phrase “This is our lane,” giving examples of work with the victims of gun violence (on a surgical gurney, for example) and noting that researching the problem is not “anti-gun” but is a necessary step to understand and address the adverse medical consequences of gun violence.22
Clinical Applications of Recent Research
“The list of what isn’t known is much longer than what is known,” said Dr. Garen Wintemute, director of the Violence Prevention Research Center, University of California, Davis, regarding evidence-based prevention of gun violence in 2013. More recently, with the potential influx of data from new studies, his outlook has become slightly more optimistic. In 2022, Dr. Wintemute said, “We are in the beginning phases of grappling with the breadth of what we still need to know.”23
Dr. Wintemute and other researchers in the field advocate for tackling gun violence by starting with the four fundamental questions included in a basic approach of public health to medical problems:23,24
1. What is the problem?
2. What are the causes?
3. What works for prevention?
4. How do we translate findings from research into clinical practice?
In early work along these lines, research sponsored by the RAND Corporation in 2018 and 2020 looked at 18 types of gun laws to determine any association with enhanced outcomes, such as a decrease in homicide, mass shootings, or police shootings, and found no strong evidence of such an association. However, the January 2023 report from the RAND Corporation shows that there is increasing (although still “modest”) evidence that some policies and laws are associated with significant benefits.19
For example, safe-storage laws are associated with reduced fatal and nonfatal self-inflicted gun injuries as well as reduced homicides using firearms among youth. There is moderate evidence from these studies that laws prohibiting domestic abusers from gun ownership are associated with reduced fatalities from domestic abuse, that waiting periods before purchasing a gun are associated with decreased firearm suicides and homicides, and that background checks are associated with a decrease in firearm homicide.19
It is important for all clinicians to know that there are no state or national laws or regulations that prohibit conversations with patients about firearms. Multiple studies have confirmed that patients generally are receptive to such discussions, especially if there is an awareness that someone in the household is at risk.25
The following section presents facts and research findings applicable to specific clinical scenarios.
Teen Patient with Risky Behaviors
B.J. is a gregarious 16-year-old, known to you from periodic well child checks and a sports physical in middle school. B.J. comes in today at the recommendation of a local mental health counselor, who became involved with B.J. after a referral from his school following a fight and being caught with alcohol in a water bottle. “My counselor thinks I’m depressed,” says B.J., “and that you could give me some pills or something to help.”
When the provider asks B.J. for some more information, B.J. replies, “Look, I don’t really want to answer all these questions or fill out forms. I am just bored at school, and I like to drink sometimes. It’s not like I am going to shoot up the cafeteria or kill myself or anything.”
The provider may want to consider the following facts in formulating a plan and direction with B.J.:
• Firearms are the leading cause of death for teens in the United States; fatalities from firearm injuries have risen by about 44% in this population since 2013. Fifty-nine percent of these are the result of homicide, 37% are from suicide, and 3% are unintentional. Non-fatal firearm injuries in this age group led to approximately 100,000 emergency department visits since 2013.1,2,26,27
• Safe-storage laws are associated with reduced self-inflicted and homicidal firearm fatalities in youth. There is evidence from several trials that counseling about safe storage of firearms combined with providing a safe-storage device increases the probability of safe firearm storage (the association with safe storage is stronger with both interventions than with either one alone). There also is evidence that most PCPs do not discuss firearm safety. In a large 2022 study surveying a nationally representative sample of caregivers of teens who had received preventive care counseling, only 14.9% confirmed that firearm safety was discussed.26-28
• Alcohol and drug use raises the risk for firearm fatalities and injuries for all ages.1,27,29
• Repeated studies have shown firearm access is the highest risk factor for teen firearm injuries. In 80% of teen firearm suicides and 90% of unintentional teen firearm fatalities, the gun was obtained from the home of the teen or the home of a relative.28
• Most suicide attempts are impulsive; decreasing access to lethal means of suicide during times of emotional upheaval or crisis (known as lethal means counseling) can be effective in prevention of completed suicides.30,31
The clinician is faced with a difficult but far from unusual situation: a 16-year-old who does not want to engage in an office interview. What makes this clinical encounter most worrisome are the unknowns and the high-risk behaviors. For example, there is not enough information to understand why the patient was fighting or drinking, if this is an acute change in behavior or had a slower onset, if there have been other behavioral or emotional changes, and why the patient has referenced guns.
Collateral information, such as from the counselor, the school, and a parent or guardian, will be needed. However, an alignment with the identified patient (B.J.) is an essential first step to move forward.32
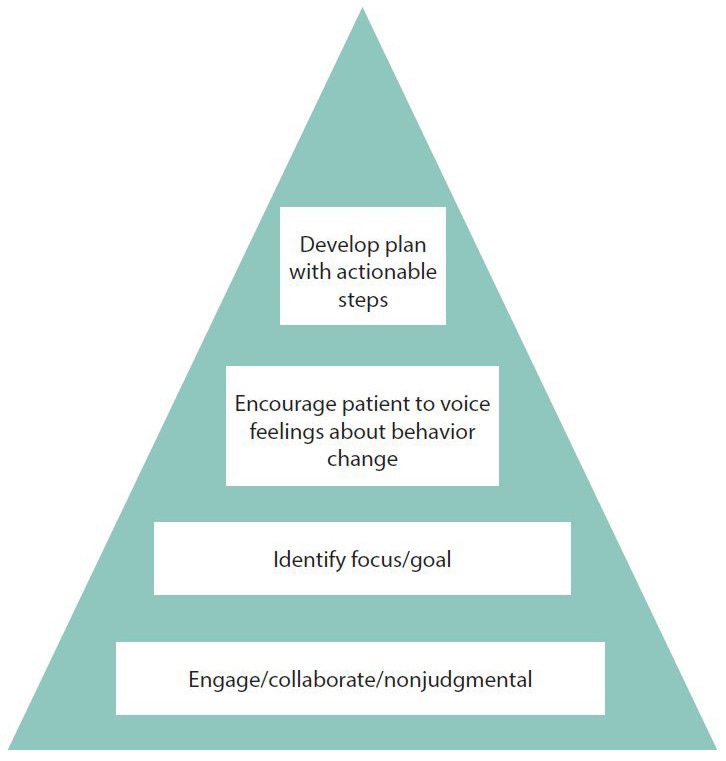
Motivational interviewing (MI), an evidence-based tool for behavioral change, is arguably the approach to the clinical interview most likely to succeed at this point. The foundation of MI rests upon understanding that our role as a provider when discussing behavioral change is not directive — we are not able to “order” change. This concept does not relegate the provider to the sidelines. Rather, the provider takes the role of a trusted partner or guide, developing empathy and assuring patient autonomy in decision-making while encouraging the patient to voice any internal motivation and desire for change.33-35
The core elements of MI (engage, identify a goal, understand readiness to change, and develop an actionable plan) are displayed in Figure 1.33-35
Figure 1. The Core Elements of Motivational Interviewing |
 |
There are several models of patient interview that apply these concepts of MI. When there appears to be motivation for change, the OARS model (an acronym for the components of the interview; see Table 1), which was developed by the founders of MI, often is used. On the other hand, “Five A’s” (another acronym; see Table 2) more often is used when motivation for change is low. The latter technique has shown promise in several studies of firearm safety counseling in primary care. In all cases, the fundamental issue of establishing a trusting connection with the patient is the initial critical step.34-36
Table 1. The OARS Model34 |
|
O |
Open-ended questions (unable to respond yes/no) Avoid “why” questions, since these can promote defensiveness. For example, a provider may ask “What bothers you most about your situation?” rather than “Why does this bother you?” since the latter format may be taken as criticism. Note that the goal is not to find a solution for the patient, but to develop empathy and understanding so the patient feels comfortable discussing the health dilemma and considering solutions. |
A |
Affirmations: Find the internal strengths of the patient and acknowledge them This fundamentally differs from praise and relies on the interviewer noting positive characteristics elicited by the interview. For example, the provider could say, “It sounds like you’ve given some thought to your situation, and I appreciate your honesty in letting me know where you stand,” the provider could say. |
R |
Reflective listening Listen carefully and voice back to the patient the concept, idea, or theme the patient is attempting to convey. |
S |
Summarizing Summarizing statements can be used midway and toward the conclusion of the interview and may take the form of, “Here is what I am hearing so far … tell me if I am leaving out any point important to you.” |
Reaching for an empathetic stance and trying to convey that the provider is listening, the provider speaks to B.J.
“I can only guess from what you are saying that you think someone along the line has overreacted to what happened at school and thought you were dangerous,” says the provider. “If that is so, I am sorry you feel that way and I can understand why you would not want to say anything now.”
“Yes,” says B.J., “you don’t have to be sorry — it’s not your fault. And I know you need to know some of what happened. I really hate to talk about it. It just makes me feel so bad — I really screwed up.”
“I get it,” says the provider, “no one wants to feel bad or blamed. I am glad you know I need some information to help you figure out your next steps. Maybe we can just start with a basic outline of what’s been happening.”
With the connection to the patient established, the provider can gather background information and learn more about what is going on with B.J. in addition to B.J.’s thoughts about guns and access to guns.
“OK,” says B.J. “But first I want you to know I would never use a gun against anyone. Ever since I got in trouble, that’s all every doctor and counselor want to talk about. And now my dad says they’re going to take our guns away and he’s not going to let that happen.”
“Well,” replies the provider, “it sure sounds like there are other things to talk about. Like getting in trouble in school with fighting and drinking. But maybe we can start with putting the gun issue to rest. Are you OK to have your dad come in and we can develop a plan for the guns so everyone feels safe?”
The provider follows B.J.’s lead in talking about the guns first. Now, with the information given, it appears that use of the Five A’s may be appropriate.
In 1989, the National Cancer Institute published a description of the “Four A’s” (ask, advise, assist, arrange) as guidelines to an approach for physicians when attempting to assist patients in stopping smoking. Over time, the “Four A’s” grew into what now is known as the “Five A’s” with the addition of “agree” midway through the process. The U.S. Preventive Services Task Force (USPSTF), as well as national agencies worldwide, promote the Five A’s approach for behavioral counseling in primary care. Several recent studies have looked at the efficacy and practical implementation (including instruction of providers) of this method of interviewing for firearm safety counseling.36,37
The Five A’s
1. Ask/Assess. Asking about health-related behaviors can be complicated. Rarely are patients coming to primary care explicitly to discuss behavior. In the case of B.J., there appears to be an element of outside coercion. Borrowing from core MI concepts, the provider will get furthest by taking a nonjudgmental stance while trying to understand the patient view of the situation. The dilemma for the clinician in this case is that there are too many “red flags” (including the mention of guns and alcohol), and implementation of almost any intervention will require the cooperation of an adult guardian. Bringing a parent or guardian in, with the permission of the minor patient, is a necessary step.32,36,37
2. Advise. Advising this patient presents some challenges and, notably, will involve not only the patient, but the guardian. An empathic, non-critical approach (as borrowed from MI) is most likely to allow the provider’s advice to be heard. Advice also is generally best accepted when paired with knowledge, such as understanding the role of the firearms for the family and having at least a basic familiarity with safe storage practices. The concept of harm reduction plays a role here as well — looking to reduce harm to an acceptable level rather than eliminate all risk.36,37
Back to B.J. and the father:
Trying to avoid phrases such as “you should” that may promote defensiveness, the provider focuses on facts and connecting behavior to unwanted outcomes, saying, “B.J. is here because the counselor wanted me to evaluate if medications would help him, and we will discuss that. But B.J. also mentioned concerns have been brought up about guns at home and that the two of you are not sure this concern is necessary. Can we talk about this?”
“No need,” says the father. “We have a small gun collection for hunting and self-defense, and really guns are just my hobby. My lawyer says no one can take them away just because B.J. has had some behavior issues.”
3. Agree. This next “A,” as with its predecessors, is more complicated under the surface than may be anticipated. Notably, this step was not included in the original Four A’s of the late 1980s. Since that time, there has been accumulating evidence on the importance of patient-provider collaboration regarding medical care in general. Consider that patient values may not be readily evident to the provider, but along with psychosocial factors, patient values affect decision-making and compliance.36,37
Coming to a collaborative goal is more likely to save time and frustration in this appointment and reach a better outcome over time.
“Well,” replies the provider, “I am not talking about forced gun removal. You are correct — that is a legal issue. I can tell you what I know about gun safety from a medical standpoint, and you may know even more as a gun collector yourself.”
“Save your breath,” says the father. “I keep all my firearms locked, unloaded, ammunition separate, and no one else knows the combination,” he continues. Both look over at B.J., who is looking at the floor. After a short moment of silence, the father continues a little slower, “But I also thought I had the alcohol under lock and key — and that didn’t work so well.” B.J. looks up.
“I kind of do know the combination to the gun safe … but I would never go in there without permission,” he says.
A 2006 rural Alabama study looking at parental misperceptions of children and firearms (and entitled the same) found that many children in the study were aware of the location of firearm storage in the home and/or had handled the firearms, despite parents’ statements to the contrary.38
4. Assist. This step may involve a range of interventions, including assistance from staff members, such as a nurse or health coach, referrals to outside providers, apps that help with monitoring or tracking behavior, and/or any other concrete method of helping the patient move toward the next step or a concrete goal.36,37
Several investigations looking at implementation of the Five A’s have shown that there is a higher likelihood of behavioral change when all steps (all Five A’s) are addressed, but that providers around the world tend to falter on the application of the “assist” and “arrange” steps. One reason for this includes provider uncertainty, such as not knowing what materials and resources are available to assist a patient in making behavioral changes.36,37
This finding highlights the importance of being connected to the region and community. Another notable finding from these studies points to organizational support as a major factor (even more critical than training) in determining if a provider applies the Five A’s method during a visit. This may range from providing staff to help with implementation to documentation support to providing brochures or other material with information about services available to reinforce desired behavioral changes.36,37
Relevant to this case, a 2022 study of the use of training clinicians in the Five A’s approach specifically for firearm safety counseling found that prior to training, 60% of the trainees (residents in psychiatry, medicine, and pediatrics) were uncomfortable to extremely uncomfortable counseling on firearm safety. This number plummeted to 4% after didactic education and participation in simulated patient scenarios. It appears that a combination of training, organizational support (which may affect training opportunities), and community resource knowledge all are key ingredients in successful gun safety counseling.36
“We raise our kids to be independent and then they do things we adults don’t particularly like,” says the provider.
B.J. notes, “I don’t really like everything I do either — especially taking your beer, Dad. I know that was wrong.”
The provider nods. “I’m glad both of you brought up the alcohol — drinking and guns are a dangerous mix.”
Says the father, “That does worry me. I guess I should change the combination on the gun locker.”
The provider adds, “We also have gun cable locks or trigger locks for free here at the clinic. You have a resourceful kid — my general recommendation, if you keep guns in the house, is to store the guns unloaded and locked and the ammunition locked up separately, just like you said. But with B.J. getting in trouble lately, have you considered taking any further steps with the guns?”
“I sure do not want to think I need to,” says the father, “but maybe I will go to the biometric safe — that way only I could get in. No combination needed.”
5. Arrange. This last step reminds the provider that behavioral changes happen over time, and follow-up appointments typically are necessary to assess the relative success of the intervention. This model can be equated with models for management of a patient being treated for any number of chronic diseases. For example, a patient starting with hypertension treatment may need several follow-up appointments to determine the efficacy of the intervention and often will need adjustment of the intervention over time.36,37
B.J. needs further evaluation; clearly, addressing the guns is only a beginning. In this case, the directive to address the guns first comes directly from B.J. (“And now my dad says they’re going to take our guns away and he’s not going to let that happen.”) This statement presents an opportunity to bring in the father and discuss gun safety and related concerns. With a basic rapport now established, further evaluation of mood, the extent of mood changes, related symptoms, and drinking and other substance use may be smoother. Collateral information (from school and the counselor, for example) most likely is needed before deciding on a definitive intervention or course of action. Making a timely follow-up appointment may be the best step.32
The basics of firearm safe storage involve promoting firearms to be stored locked, unloaded, and with ammunition in a separate location. When there are elevated risks for self-harm, it is reasonable to intensify these efforts either by more complex storage practices or even a temporary removal of the firearms from the home.36,39
One more note on B.J.: When interacting with patients and families, it is useful to be mindful of unconscious biases that could affect the approach or treatment direction. In this case, B.J.’s identifying characteristics, such as gender, race, and socioeconomic level, have been removed from the clinical example. This encourages providers to ask themselves if any of these factors would affect their level of concern or the direction of the interaction with B.J. and B.J.’s father.
A recent cross-sectional study looking at the demographics of gun violence fatalities in the United States found significant and increasing variation in fatality rates according to gender, race, and ethnicity over time.40
This study and others (such as the CDC) noted that males of all ages are at a 10-fold higher risk of gun death via homicide and suicide compared to females, that Black males are at particularly high risk for homicide via firearm, and that suicide via firearm is most common in rural compared to urban and suburban areas.40,41
Adult Patient with Depression
S.L., a retired physician, 82 years of age, is well known to you for treatment of hypertension (lisinopril 20 mg daily), depression (fluoxetine 20 mg), and chronic low back pain (non-steroidal anti-inflammatory drugs). He comes today for a recheck, stating that his sleep has been “getting worse” and he is getting forgetful. His wife, who is with him, mentions that he is more irritable and he has been drinking at night when he cannot sleep. On interview, he notes that his mood has been “up and down.” When asked about suicidal thoughts, he states, “Sometimes it seems like a good idea — I think I understand why people do that. But I don’t think I have the guts.”
The provider may want to consider the following facts in formulating a plan and direction with S.L.:
• According to the CDC, people aged 85 years and older have the highest rate of suicide at 20.9/100,000, followed by those aged 75 to 84 years, at 18.9/100,000. To put these figures into perspective, the annual average age-adjusted suicide rate in the United States is 13.5/100,000 individuals.42
• Suicide is the 11th leading cause of death in the United States. Although only 5% of attempts are via firearms, more than half of completed suicides are via firearm.1,41
• Risk factors for suicide include a history of mental illness (such as depression), chronic pain, dementia, and alcohol use disorder.1,3,29
• As mentioned earlier, most suicide attempts are impulsive, with a decision to act within one hour of the action in 71% of the cases. Decreasing access to lethal means of suicide can save a life; 90% of people who survive a suicide attempt do not go on to complete suicide in the future.30,31
Thinking about risk factors, knowing that medical studies have confirmed that most adults do not mind being asked about access to firearms, and using some of the principles of MI, the provider notes:42
“You must be feeling lousy if sometimes suicide seems like a good idea. I am glad to hear you would not act on your thoughts. But tell me more about what you mean when you say you wouldn’t have the guts.”
“Well,” replies S.L., “to shoot myself, I mean. Sometimes I just look at my rifle and wonder if I could ever turn around and use it on myself. I just don’t know how people do that — but, you know, my friend did it not too long ago with a handgun. I don’t even know if you can use a rifle to kill yourself.”
His wife interjects, “I keep telling him he should get rid of those guns.”
The provider has several options here, but all lead to the same place — removing the most lethal means of suicide from the household while evaluating the degree of depression, sleep disturbance, and any evidence of cognitive decline and coming to a better understanding of the escalation in drinking.
Notably, even if there is a thought that S.L. requires hospitalization to better address these issues, the concept of reducing lethal means of suicide remains a top priority (given that S.L. most likely would be discharged home at some point).30,31
There are several pathways for counseling about securing firearms. In general, the first step is to have an open discussion regarding safe storage of the guns (unloaded, locked, and away from the locked ammunition), both to prevent unintentional use and to reduce the likelihood of an impulsive act of self-harm. This can be individualized according to the primary use for the firearms (for example, storage techniques will look different for someone worried about self-defense vs. a hunter).36,39
However, with S.L. stating that he has had thoughts regarding use of the firearms for suicide, and with S.L. drinking more and perhaps experiencing a cognitive decline, further steps are indicated.
“I am not getting rid of my guns,” replies S.L. to his wife. “That is off the table.”
“Well,” says the provider, “I hear you value your guns, but I also hear your wife is worried. Have you considered any way to reassure her that you will be safe?”
After a pause, S.L. slowly begins, “I guess I could give her the keys to the gun cabinet. Actually,” he continues, “I think that would make me feel safer, also.”
His wife looks up. “To tell the truth,” she says, “the kids called last week and want to come over and take the ammunition. They are scared, too. I think if I hold on to the keys and you give them the ammunition, that will help everyone sleep better.”
“Maybe even me,” replies S.L.
It is useful to have a basic familiarity with state laws regarding transfer of firearms. In some states, family members, gun dealers, and/or law enforcement can store guns temporarily on a voluntary basis when there are concerns about the mental stability of a household member of the gun owner. In other states, there may be some restrictions on this process. A 2017 Journal of the American Medical Association article, “Temporary Transfer of Firearms from the Home to Prevent Suicide — Legal Obstacles and Recommendations,” gives a state-by-state overview of the requirements for background checks and/or other legal steps for temporary transfer of firearms for safety. In all cases, the person willing to receive the firearm must be older than 18 years of age and able to store the firearm in a safe manner.43 (See Table 2 for a sample of online resources for clinicians.)
Table 2. A Sample of Online Tools Useful to Clinicians |
|
Website |
Notes |
Developed by researchers from the University of Colorado, Anshutz, Lock2Live is a free, interactive web-based decision-making tree focusing on reducing intentional self-harm from guns or medications. Lock2Live has shown promise with safety planning for adults in the emergency room and for outpatients with suicidal ideation. |
|
Developed by physicians for medical providers and mental health clinicians to “provide clinical tools for firearm injury prevention.” Includes a free 60-minute CME course. |
|
https://mededucation.stanford.edu/courses/physicians-and-firearms2020/ |
Clinicians and Firearms: A curriculum on firearm injury prevention in medical practice. The free CME course was developed by medical students. |
As an aside, although it may be thought that handguns are the only firearms used in suicides, it turns out that long guns, such as rifles and shotguns, also have a role in this epidemic. A 2018 study from Maryland revealed a surprising 28.4% of completed firearm suicides over 15 years were from long guns (with a disproportionate amount from rural areas and in youth).44
In this case, if S.L. was not willing to cooperate in the safety measures discussed, more stringent intervention may be considered. State laws differ in this respect; it is important to have a basic knowledge of the civil commitment procedures when working with any suicidal patient. If a patient does not meet criteria for an involuntary commitment from a mental health standpoint, but there is a concern for gun violence, a gun violence restraining order or extreme risk protection order (also known as a “red flag” order) may be pursued. These are temporary civil court orders to remove firearms and ban the purchase of additional firearm-related materials when there is evidence of firearm-related risks (with or without a mental health diagnosis).44,45
A Word About Alcohol and Gun Violence
“Never use alcohol, over-the-counter drugs, or prescription drugs before or while shooting,” according to firearm safety rules published on the NRA website.46 A growing body of evidence supports the connection between misuse of substances and gun violence, including a large-scale 2016 comprehensive review and meta-analysis revealing alcohol use as a modifiable risk factor for death by firearms.47 More recent studies have found an association between conviction of driving under the influence and gun-related violent crimes or actions.48
In 2022, Cerda et al published a simulated model prohibiting gun purchases by individuals convicted of alcohol or substance-related misdemeanors. This action resulted in a small (but significant) decrease in firearm-related homicides and suicides at population level.49 While more research is needed to fully understand the relationship, the clinician is on solid ground recognizing that misuse of substances — including alcohol — is associated with the risk of firearm violence among gun owners.
Summary/Take-Home Points
• Reducing gun violence is a public health priority.
• One-third of homes in the United States have firearms.
• Of firearm fatalities, 58.8% are from intentional self-harm.
• Counseling regarding safe storage and/or lethal means reduction can save lives; most suicide attempts are impulsive, and most individuals who survive a suicide attempt do not go on to complete a suicide later.
• Safe storage of firearms includes locked and unloaded guns with ammunition locked separately.
• MI techniques and the Five A’s are useful tools when counseling patients about safety and firearms.
• Consider risk factors (including age, cognitive status, substance misuse history, and availability of firearms) when working with patients who own guns and consider harm-reducing interventions.
References
- Gramlich J. What the data says about gun deaths in the U.S. Pew Research Center. Published April 26, 2023. https://www.pewresearch.org/fact-tank/2022/02/03/what-the-data-says-about-gun-deaths-in-the-u-s/
- Kaufman EJ, Delgado MK. The epidemiology of firearm injuries in the US: The need for comprehensive, real-time, actionable data. JAMA 2022;328:1177-1178.
- Conner A, Azrael D, Miller M. Suicide case-fatality rates in the United States, 2007-2014: A nationwide population-based study. Ann Intern Med 2019;171:885-895.
- McGough M, Amin K, Panchal N, Cox C. Child and teen firearm mortality in the U.S. and peer countries. KFF Global Health Policy. Published July 8, 2022. https://www.kff.org/global-health-policy/issue-brief/child-and-teen-firearm-mortality-in-the-u-s-and-peer-countries/
- American Public Health Association. Violence is a public health issue: Public health is essential to understanding and treating violence in the U.S. Published Nov. 13, 2018. https://apha.org/policies-and-advocacy/public-health-policy-statements/policy-database/2019/01/28/violence-is-a-public-health-issue
- Berkowitz L, Macaulay J. The contagion of criminal violence. Sociometry 1971;34:238-260. https://www.jstor.org/stable/2786414
- Bloomfield MA, McCutcheon RA, Kempton M, et al. The effects of psychosocial stress on dopaminergic function and the acute stress response. Elife 2019;8:e46797.
- Forum on Global Violence Prevention; Board on Global Health; Institute of Medicine; National Research Council. Contagion of Violence: Workshop Summary. National Academies Press; 2013.
- Slutkin G, Ransford C, Zvetina D. Response to “metaphorically or not, violence is not a contagious disease.” AMA Journal of Ethics. Published May 2018. https://journalofethics.ama-assn.org/article/response-metaphorically-or-not-violence-not-contagious-disease/2018-05
- Slutkin G. Why we need to treat violence like a contagious epidemic. The Guardian. Published Jan. 13, 2020. https://www.theguardian.com/us-news/commentisfree/2020/jan/13/changing-violence-requires-the-same-shift-in-understanding-given-to-aids
- Hoops K, Fahimi J, Khoeur L, et al. Consensus-driven priorities for firearm injury education among medical professionals. Acad Med 2022;97:93-104.
- Sanders RS Jr. Dr. Seat Belt: The Life of Robert S. Sanders, MD, Pioneer in Child Passenger Safety. Armstrong Valley Publishing; 2008.
- American Academy of Pediatrics. Gun safety and injury prevention. Last updated July 27, 2022. https://www.aap.org/en/patient-care/gun-safety-and-injury-prevention/
- Fox K, Shveda K, Croker N, Chacon M. How US gun culture stacks up with the world. CNN. Updated April 10, 2023. https://www.cnn.com/2021/11/26/world/us-gun-culture-world-comparison-intl-cmd/index.html
- ProCon.org. History of gun control. Last updated March 20, 2023. https://gun-control.procon.org/history-of-gun-control/
- Morgan T. The NRA supported gun control when the Black Panthers had the weapons. The History Channel. Updated Aug. 31, 2018. https://www.history.com/news/black-panthers-gun-control-nra-support-mulford-act
- Kellerman AL, Rivara FP, Rushforth NB, et al. Gun ownership as a risk factor for homicide in the home. N Engl J Med 1993;329:1084-1091.
- Roubein R, Beard M. Now the government is funding gun violence research, but it’s years behind. The Washington Post. Published May 26, 2022. https://www.washingtonpost.com/politics/2022/05/26/now-government-is-funding-gun-violence-research-it-years-behind/
- RAND Corporation. Gun policy in America. https://www.rand.org/research/gun-policy.html
- Ault A. Gun violence researchers are making up for 20 years of lost time. JAMA 2021;326:687-689.
- South EC, Hemenway D, Webster DW. Gun violence research is surging to inform solutions to a devastating public health crisis. Prev Med 2022;165(Pt A):107325.
- American Foundation for Firearm Injury Reduction in Medicine. #ThisIsOurLane. https://affirmresearch.org/this-is-our-lane
- UC Davis Health. Violence Prevention Research Program. https://health.ucdavis.edu/vprp/
- The Educational Fund to Stop Gun Violence. The public health approach to gun violence prevention. Published November 2020. https://efsgv.org/wp-content/uploads/PublicHealthApproachToGVP-EFSGV.pdf
- McCourt AD, Vernick JS. Law, ethics, and conversations between physicians and patients about firearms in the home. AMA J Ethics 2018;2069-2076.
- Lee LK, Fleegler EW, Goyal MK, et al. Firearm-related injuries and deaths in children and youth. Pediatrics 2022; Oct 8. doi 10.1542/peds.2022-060071. [Online ahead of print].
- Rowhani-Rahbar A, Simonetti JA, Rivara FP. Effectiveness of interventions to promote safe firearm storage. Epidemiol Rev 2016;38:111-124.
- Seewald LA, Myers M, Zimmerman MA, et al. Firearm safety counseling among caregivers of high-school age teens: Results from a national survey. Prev Med 2022;165(Pt A):107285.
- McGinty EE, Webster DW. The roles of alcohol and drugs in firearm violence. JAMA Intern Med 2017;177:324-325.
- Centers for Disease Control and Prevention. Suicide prevention: Risk and protective factors. https://www.cdc.gov/suicide/factors/index.html#factors-protect
- Harvard T.H. Chan School of Public Health. Duration of suicidal crises. https://www.hsph.harvard.edu/means-matter/means-matter/duration/
- Zuckerbrot RA, Cheung A, Jensen PS, et al. Guidelines for Adolescent Depression in Primary Care (GLAD-PC): Part I. Practice preparation, identification, assessment, and initial management. Pediatrics 2018;141:e20174081.
- Motivational Interviewing Network of Trainers. Understanding motivational interviewing. https://motivationalinterviewing.org/understanding-motivational-interviewing
- Haque SF, D’Souza A. Motivational interviewing: The RULES, PACE, and OARS. Current Psychiatry 2019;18:27.
- Alqarni MA. Counselling style through motivational interviewing – A tool for clinicians: A review. Ann Med Health Sci Res 2019;9:550-552.
- Hoops K, McCourt A, Crifasi CK. The 5 A’s of firearm safety counseling: Validating a clinical counseling methodology for firearms in a simulation-based randomized controlled trial. Prev Med Rep 2022;27:101811.
- Crifasi C, Hoops K. The 5A’s of firearm safety counseling. CLOSLER: A Miller Coulson Academy of Clinical Excellence Initiative. John Hopkins Medicine. Published Jan. 22, 2019. https://closler.org/lifelong-learning-in-clinical-excellence/the-5as-of-firearm-safety-counseling#:~:text=Implementation%20of%20the%205A's%20model,weight%20loss%20among%20obese%20patients
- Baxley F, Miller M. Parental misperceptions about children and firearms. Arch Pediatr Adolesc Med 2006;160:542-547.
- Pallin R, Barnhorst A. Clinical strategies for reducing firearm suicide. Inj Epidemiol 2021;8:57.
- Rees CA, Monuteaux MC, Steidley I, et al. Trends and disparities in firearm fatalities in the United States, 1990-2021. JAMA Netw Open 2022;5:e2244221.
- Centers for Disease Control and Prevention. Fast Facts: Firearm violence prevention. Last reviewed May 4, 2022. https://www.cdc.gov/violenceprevention/firearms/fastfact.html
- Wintemute GJ, Betz ME, Ranney ML. Yes, you can: Physicians, patients, and firearms. Ann Intern Med 2016;165:205-213.
- McCourt AD, Vernick JS, Betz ME, et al. Temporary transfer of firearms from the home to prevent suicide: Legal obstacles and recommendations. JAMA Intern Med 2017;177:96-101.
- Nestadt PS, MacKrell K, McCourt AD, et al. Prevalence of long gun use in Maryland firearm suicides. Inj Epidemiol 2020;7:4.
- Fairbank R. How red flad laws reduce risks of gun violence. Hub: John Hopkins University. Published July 11, 2022. https://hub.jhu.edu/2022/07/11/how-do-extreme-risk-protection-orders-work/
- National Rifle Association. NRA gun safety rules. https://gunsafetyrules.nra.org
- Branas CC, Han S, Wiebe DJ. Alcohol use and firearm violence. Epidemiol Rev 2016;38:32-45.
- Kagawa RM, Stewart S, Wright MA, et al. Association of prior convictions for driving under the influence with risk of subsequent arrest for violent crimes among handgun purchasers. JAMA Intern Med 2020;180:35-43.
- Cerdá M, Hamilton AD, Tracy M, et al. Would restricting firearm purchases due to alcohol- and drug-related misdemeanor offenses reduce firearm homicide and suicide? An agent-based simulation. Inj Epidemiol 2022;9:17.
Gun violence is a leading cause of premature death in the United States. More than 45,000 Americans died from gun violence in 2020, a substantial increase from previous years. The scope of the problem is such that the American Public Health Association has identified gun violence as a public health problem and recommends a “comprehensive public health approach.” Primary care providers (PCPs) are in a unique position to lead the way in a campaign to reduce harm from firearms.
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.