By Lisa Mosconi, PhD
Associate Professor of Neuroscience in Neurology and Radiology, Weill Cornell Medicine
SYNOPSIS: Two independent analyses of U.S. national surveys support evidence that targeted risk-reduction strategies may reduce the burden of Alzheimer’s disease in the population.
SOURCES: Nianogo RA, Rosenwohl-Mack A, Kristine Yaffe K, et al. Risk factors associated with Alzheimer disease and related dementias by sex and race and ethnicity in the US. JAMA Neurol 2022;79:584-591.
Lee M, Whitsel E, Avery C, et al. Variation in population attributable fraction of dementia associated with potentially modifiable risk factors by race and ethnicity in the US. JAMA Netw Open 2022;5:e2219672.
Alzheimer’s disease (AD) is the most common cause of dementia, accounting for 60% to 80% of all dementia cases. As the baby boomer generation ages, the number of people living with dementia is projected to increase from 5.8 million in 2020 to 13.8 million by 2050.1 The prevalence of AD is higher in women than in men, with post-menopausal women accounting for nearly two-thirds of all cases.1 The prevalence of dementia is twice as high among non-Hispanic Black individuals and 1.5 times as high among Hispanic individuals as compared with non-Hispanic white individuals.1
Currently, there are no pharmaceuticals to prevent or slow the progression of AD and related dementias. In the absence of disease-modifying treatments, identifying and managing potentially modifiable risk factors for AD is crucial to address the projected increase in prevalence.
In the last 10 years, population-based observational studies and randomized clinical trials have identified several potentially modifiable risk factors for AD and estimated the fraction of global dementia cases associated with these risks. In 2020, the Lancet Commission summarized the available evidence, highlighting 12 risk factors most likely to be causally related to dementia.2 These include low education, hearing loss, traumatic brain injury (TBI), hypertension, excessive alcohol consumption, obesity, smoking, depression, social isolation, physical inactivity, diabetes, and air pollution. The report estimates that these risks may account for up to 40% of all dementia cases globally, which could, therefore, have been prevented by means of risk-reduction interventions.
In an effort to update these estimates with more recent data, Lee et al analyzed four cross-sectional U.S. national surveys to estimate the fraction of dementia cases associated with the 12 modifiable risks noted earlier.3 Surveys included the American Community Survey, the National Health and Nutrition Examination Survey, the National Health Interview Survey, and the National Social Life, Health, and Aging Project. To estimate exposure to air pollution, they used census estimates of air quality from the Center for Air, Climate, and Energy Solutions. Among the total U.S. population, the risk factors associated more consistently with dementia were midlife hypertension and obesity (20.1% and 20.9%, respectively), and late-life physical inactivity (20.1%). An aggregated 41% of dementia cases in the U.S. population were associated with all 12 potentially modifiable risks.
The authors also examined population attributable fractions (PAFs) for each risk factor alone and in combination with the others, taking into account separate racial and ethnic groups. According to these calculations, a 15% decrease in each risk factor would reduce dementia prevalence in the population by an estimated 7.3%. As shown Figure 1, the estimated cumulative PAF was greater for Black and Hispanic than for white and Asian people.
Figure 1. Unweighted Populations Attributable Fractions (PAFs) for Each Risk Factor by Race and Ethnicity |
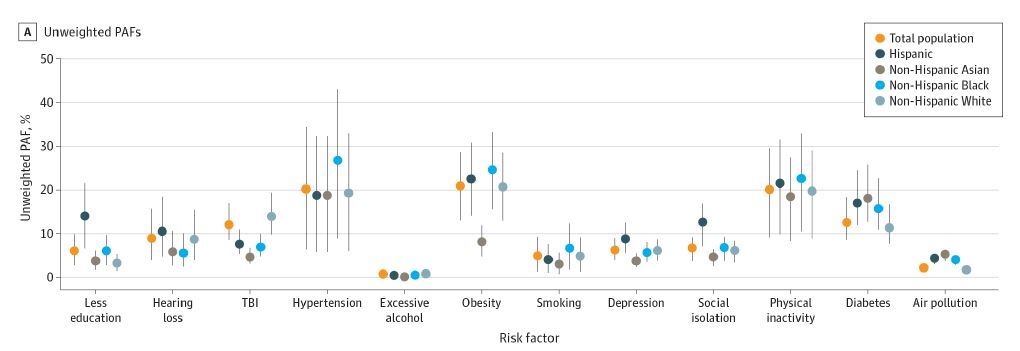 |
Source: Lee M, Whitsel E, Avery C, et al. Variation in population attributable fraction of dementia associated with potentially modifiable risk factors by race and ethnicity in the US. JAMA Netw Open 2022;5:e2219672. |
These findings are consistent with an independent report by Nianogo et al, in which the prevalence of eight modifiable risk factors for AD and related dementias was estimated from the nationally representative U.S. Behavioral Risk Factor Surveillance System Data.4 These risks included physical inactivity, smoking, depression, low education, diabetes, midlife obesity, midlife hypertension, and hearing loss. The authors stratified data by sex as well as race and ethnicity.
These eight risk factors were found in more than one-third (37%) of all dementia cases. The most common risks were midlife obesity (18%), physical inactivity (12%), and low educational attainment (12%). As shown in Figure 2, midlife obesity was the most prevalent risk for both men and women. Nonetheless, men exhibited a higher cumulative prevalence of risk than women (36% vs. 30%), except for depression, which was more prevalent in women than in men (11% vs. 6%).
Figure 2. Sex-Specific Weighted Prevalence for Each Modifiable Risk Factor Using the US Behavioral Risk Factor Surveillance System (BRFSS) Data, 2018 |
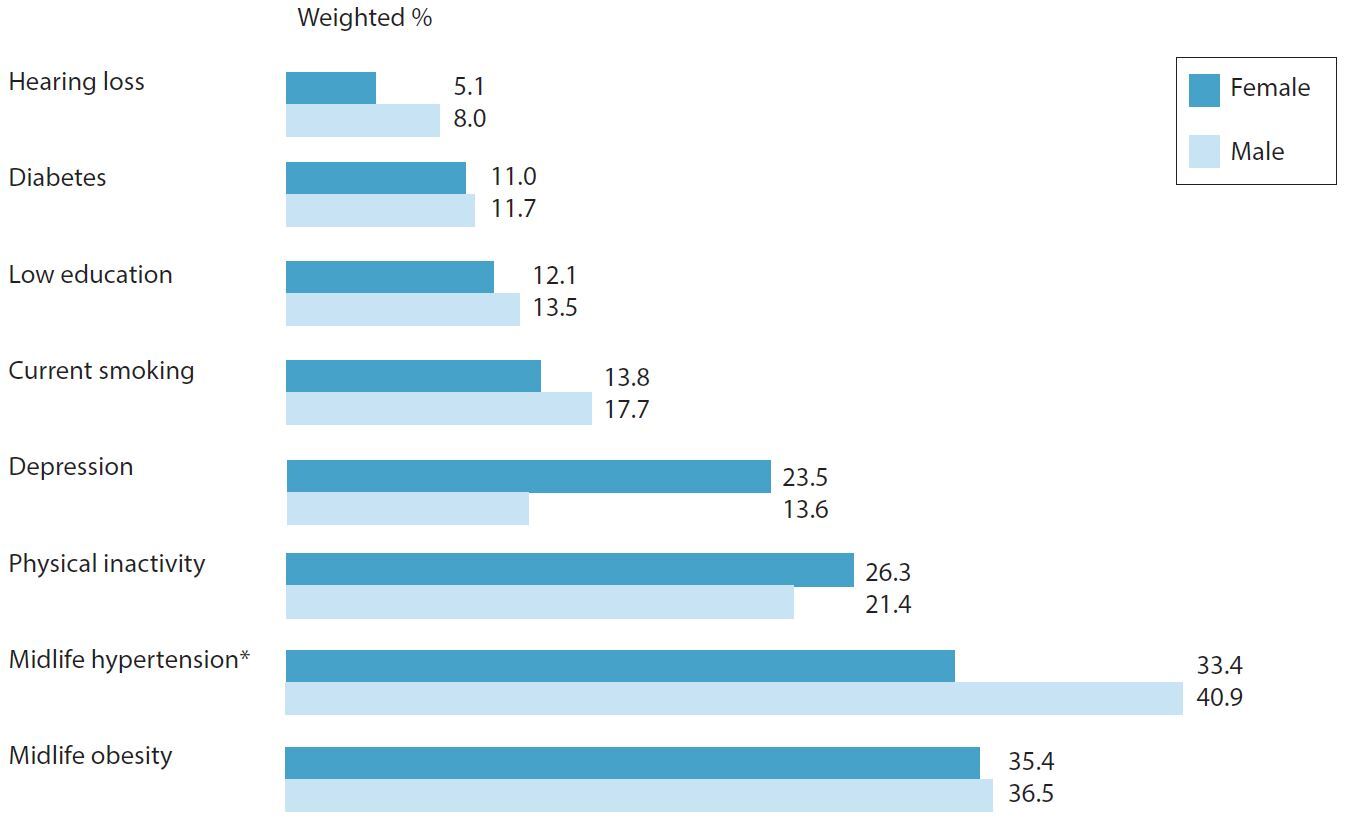 |
* Midlife hypertension data were collected in 2017 because information on hypertension was not recorded in the 2018 survey. Adapted from: Nianogo RA, Rosenwohl-Mack A, Kristine Yaffe K, et al. Risk factors associated with Alzheimer disease and related dementias by sex and race and ethnicity in the US. JAMA Neurol 2022;79:584-591. |
Among different racial and ethnical groups, the most prominent modifiable risk factors were midlife obesity for Black, American Indian, Alaska Native, and white individuals; low education for Hispanic individuals; and physical inactivity for Asian individuals. The authors estimated that a 15% proportional reduction in risk factor prevalence would be associated with approximately 427,000 fewer dementia cases in the U.S. population.
COMMENTARY
Although age is the strongest known risk factor for dementia, AD is not an inevitable consequence of biological aging or genetics. Current population-based estimates from epidemiological studies and meta-analyses have provided evidence that the prevalence of dementia could be reduced by targeting modifiable risk factors for AD and related dementias. The Lancet Commission identified 12 major risks, which include low education, hearing loss, TBI, hypertension, excessive alcohol consumption, obesity, smoking, depression, social isolation, physical inactivity, diabetes, and air pollution.
In response to the increasing number of AD cases, the U.S. federal government has set a goal to prevent and treat dementia by 2025. Additionally, the Risk Reduction Subcommittee of the National Alzheimer Project Act Advisory Council set a goal of reducing dementia risk factors in the general population by 15%.5 To achieve these goals, it is important to clarify the prevalence and relative distribution of potentially modifiable AD risk factors in the U.S. population. In both studies reviewed here, several modifiable risk factors for AD were associated with 41% and 37% of dementia cases in the U.S. population, respectively.
In the study by Lee et al, the top three risks associated with dementia were midlife hypertension, midlife obesity, and late-life physical inactivity.3 In the study by Nianogo et al, the top three risks were midlife obesity, physical inactivity, and low education.4 Therefore, midlife obesity emerged as the strongest risk factor for dementia in the population, followed by physical inactivity, which strongly argues for interventions aimed at keeping body weight within normal limits by engaging in regular exercise. Obesity was particularly prevalent among Black individuals, especially men.
A caveat: The relative risk estimates in these studies were derived from observational data. More work is needed to test whether intervening on these exposures actually lowers dementia risk. In some randomized clinical trials, mainly the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER), a multidomain intervention addressing diet, physical activity, cognitive training, and vascular risk management was associated with improved cognitive function among older adults.6 However, other clinical trials have yielded mixed results.6
Although more work is needed to conclusively determine the efficacy of risk-reduction strategies for AD prevention, physicians have an important role to play in encouraging patients to adopt a healthy lifestyle to support cognitive function, which is a crucial first step in reducing the overall burden of AD.
REFERENCES
- [No authors listed]. 2021 Alzheimer’s disease facts and figures. Alzheimers Dement 2021;17;327-406.
- Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020;396:413-446.
- Lee M, Whitsel E, Avery C, et al. Variation in population attributable fraction of dementia associated with potentially modifiable risk factors by race and ethnicity in the US. JAMA Netw Open 2022;5:e2219672.
- Nianogo RA, Rosenwohl-Mack A, Kristine Yaffe K, et al. Risk factors associated with Alzheimer disease and related dementias by sex and race and ethnicity in the US. JAMA Neurol 2022;79:584-591.
- Office of the Assistant Secretary for Planning and Evaluation. Public Members of the Advisory Council on Alzheimer’s Research, Care and Services: 2021 Recommendations. https://aspe.hhs.gov/sites/default/files/documents/18454de4f0f9ef42dacef6ef167b1933/napa-2021-public-member-recommendations.pdf
- Kivipelto M, Mangialasche F, Ngandu T. Lifestyle interventions to prevent cognitive impairment, dementia and Alzheimer disease. Nat Rev Neurol 2018;14:653-666.
Two independent analyses of U.S. national surveys support evidence that targeted risk-reduction strategies may reduce the burden of Alzheimer’s disease in the population.
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.