EXECUTIVE SUMMARY
Lifestyle choices have a significant effect on cardiovascular disease prevalence as well as outcomes.
- Lifestyle is a critical determinant of the common risk factors for cardiovascular disease (hypertension, diabetes, hyperlipidemia, and smoking) that have been well-known to predict disease outcomes.
- Lifestyle modifications can be used in conjunction with traditional medications to provide the best care to patients.
- With the dual epidemics of obesity and type 2 diabetes, an aging population, and increased population growth, lifestyle modification stands as the most cost-effective way to manage population health.
- Medical providers need to act now to prevent being overwhelmed with the eventual increase in coronary artery disease following the obesity/diabetes epidemic.
Introduction
Cardiovascular disease (CVD) is the leading cause of death globally and in the United States.1,2 According to the Centers for Disease Control and Prevention (CDC), one person dies every 33 seconds in the United States from CVD; thus, identifying and targeting cardiovascular risk factors is essential for the prevention and long-term management of CVD.3,4 Traditionally, factors for the onset and progression of CVD were thought to be mostly genetic. It is now well established that several of these factors are lifestyle mediated.
Behavioral changes significantly influence the interplay between a healthy lifestyle and the genetic risk of heart disease, as demonstrated in a study of three large prospective cohorts. In this study, a polygenic risk score determined the genetic risk, while a scoring system was used to measure a favorable lifestyle. A favorable lifestyle was defined as three of four factors (no current smoking, no obesity, regular physical activity, and a healthy diet). A favorable lifestyle was associated with a 50% decreased risk of CVD across all groups, including the highest genetic risk group.5 Furthermore, genetics explains only 7% of human longevity, as was seen in the public ancestry website study, where an ideal lifestyle could add up to 14 years of life for women and 12 years of life for men.6,7
To further understand our challenges with preventing and reversing CVD, providers need to consider the alarming prevalence of risk factors among the U.S. population. For example, hypertension (blood pressure [BP] > 130/80 mmHg) affects approximately 50% of U.S. adults, and only one in four adults have controlled hypertension.8-10 The CDC estimates that 14.7% of all U.S. adults have diabetes, and at least 3.4% of all U.S. adults who met the criteria for diabetes were not aware of this diagnosis. In addition, 38% of the U.S. population has prediabetes based on their fasting glucose or A1c level. Of those individuals with prediabetes, only 19% reported being told by a provider that they had the condition.11
The National Health and Nutrition Examination Survey (NHANES) reported that 36.7% of U.S. adults had hyperlipidemia.12 Of those, 55.5% took a cholesterol-lowering medication, and 46.6% reported making lifestyle modifications to lower their cholesterol. Only 9.5% of patients had low-density lipoprotein (LDL) levels below 70 mg/dL.12 Interestingly, 93% of those patients were on medication, with 57% also making lifestyle modifications. Another 26.9% had LDL levels between 70 mg/dL and 100 mg/dL, with 74% taking medications and 50% using lifestyle changes. The overall total control rate was only 36.4%.12
Obesity is an epidemic in the United States that began in the 1980s and is associated with the increased production and consumption of ultra-processed food, sugar, and sugar-sweetened beverages.13 It increases the risk of diabetes, stroke, and heart disease. Currently, the growing availability of pharmacologic treatment for overweight and obesity in adults has excited the medical community. However, experts and recent studies suggest that most patients can regain most of their weight within one to five years of stopping the drug.14,15 Weight gain has been attributed to numerous factors, most importantly persistent unhealthy behaviors. We need to recognize that there is a limit to what medications can help control in the setting of harmful habits, such as overeating and inadequate physical activity.
The overall population rates of risk factor prevalence and control are overwhelmingly elevated. The lone exception is smoking, which has declined. The 2016 National Health Interview Survey estimated that cigarette smoking in U.S. adults decreased from 20.9% to 15.5% between 2005 and 2016.16 However, the upsurge in vaping and marijuana use may reverse this trend, since these are recognized gateways to tobacco smoking.
Another major concern is related to medication adherence. A study examining statin adherence found that pharmacy refill rates were only 79% in post-myocardial infarction (MI) patients, 67% in patients with diabetes, and 63% in patients without diabetes and CVD.17 Another study noted that women, minorities, and younger and older adults were less likely to adhere to statins.18 Medication non-adherence could be associated with misinformation on the internet, not understanding of the effects of the medication, and distrust of large pharmaceutical companies. (See Table 1.)
Table 1. Comparative Effectiveness and Safety of Lifestyle Medicine and Traditional Pharmacotherapy |
|
Traditional Pharmacotherapy |
Lifestyle Medicine |
Pros
Cons
|
Pros
Con
|
The affordability or cost of prescribed medication is a known limiting barrier for medication adherence. A recent study showed that one in five older adults experience cost-related medication non-adherence.19 Likewise, the ARTEMIS trial evaluated if vouchers to cover the copay for P2Y12 inhibitors would increase adherence. It showed only a 3.3% absolute increase in medication adherence but no reduction of major cardiovascular events.20
A different perspective is to consider if patients are more adherent to their medications when provided optimal conditions and after a major cardiovascular event. A meta-analysis including the COURAGE, BARI 2D, and FREEDOM studies showed poor control of risk factors for coronary artery disease (CAD) secondary prevention. The metrics included the measurement of one-year goals for LDL, BP, hemoglobin A1c (HbA1c), and smoking. The percentage of patients reaching all four metrics ranged from less than 10% in the FREEDOM trial to just under 50% in the COURAGE trial. This is not very encouraging, since clinical trials are optimal environments for follow-up care.21
The REGARDS study showed suboptimal risk factor control among patients with stable CAD. The researchers measured low-dose aspirin use, non-smoking status, body mass index (BMI), physical activity, lipid management, and BP control. Unfortunately, less than 1% of participants achieved all seven risk factor goals. Furthermore, socioeconomic factors, including low income, less education, and poor functional status, were associated with fewer goals achieved.22 Another reason could be that, in medical practice, the focus remained on medication prescription rather than a combined effort of promoting healthy lifestyle behavior, tracking those behaviors, and appropriate medical management.
The American Heart Association (AHA) developed the “Life’s Simple 7” (LS7), which consists of seven health predictors of heart health as an effort to achieve ideal cardiovascular health. The health metrics include control of BP, blood glucose management, reduction of lipids, physical activity, BMI, healthy diet, and smoking cessation. In 2022, the AHA included sleep as part of the health metrics and psychological factors. Previous studies showed that less than 2% of the population had all risk factors optimized with medications and lifestyle.23
Patients with stroke have similar poor health metrics. In a study using the AHA initial LS7 metrics, researchers found that only a single patient (not 1%, but a single patient) out of 67,514 total patients had all seven ideal metrics.23 Addressing these metrics is extremely important, since investigators estimated that the worldwide risk of stroke for those older than age 25 years is approximately 25%.24 There is much work to do in the medical community and patient population to change these statistics. When looking for comprehensive lifestyle change post-infarct or post-stroke, only 4% of patients will modify their diet, exercise more, and stop smoking after a life-
changing event.25
Today, when technology and science are quickly advancing, we expect that the knowledge acquired by clinicians will be translated into tools to help close the gap between patients and their habits. Surprisingly, one of the most important reasons physicians refrain from routinely discussing lifestyle behaviors with patients is a knowledge gap in medical training. A survey of cardiovascular fellows and attendings found that the majority had little to no training in nutrition during medical school (31%), residency (59%), or fellowship (90%). Although 95% believed that dietary interventions were important, only 8% described themselves as experts in nutrition.26
Taken from the opposite perspective, authors of another study found that deficient levels of lifestyle advice were given to overweight patients (only 21.4%), and only 44.2% of obese patients received any lifestyle counseling.27 Could this be the result of providers feeling uncomfortable discussing these topics, the short time for office visits, and the belief that patients would not or could not change? Despite the growing evidence of the effect of a healthy lifestyle in preventing and reversing CVD, it is concerning that patients are not being educated on this subject. The most important reason likely is that physicians believe lifestyle modification does not work and that medications are superior. The rest of this article will focus on advocating and providing resources to reduce the knowledge gap. (See Figure 1.)
Figure 1. Factors Contributing to Development of Cardiovascular Disease |
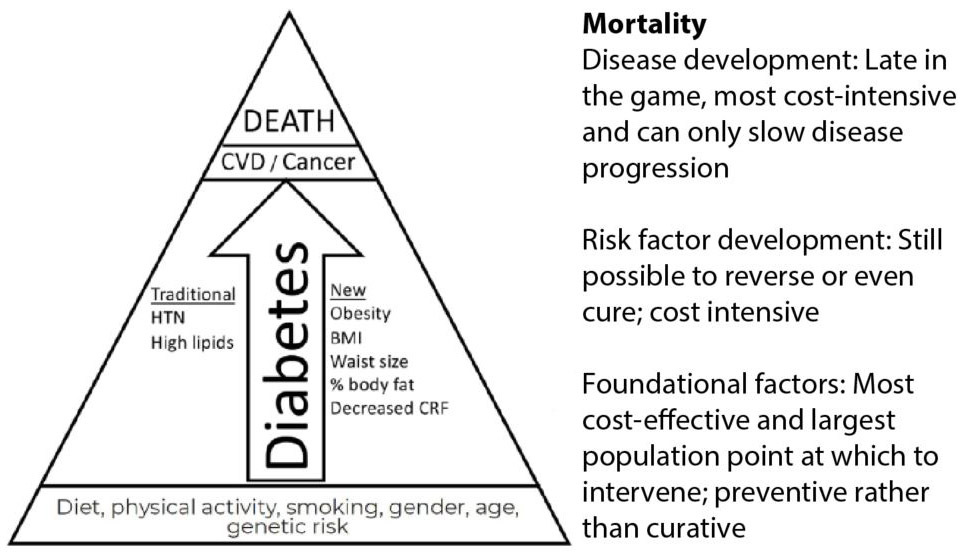 |
CVD: cardiovascular disease; HTN: hypertension; BMI: body mass index; CRF: cardiorespiratory fitness |
Treating the Cause
Even if individuals could achieve perfect health metric goals for their BP, lipids, and diabetes through medication, they would remain hypertensive, hyperlipidemic, and diabetic. Lifestyle modification provides the only way to possibly reverse these conditions. Although this might not always result in a cure, striving for that goal will improve their outcomes and long-term management of disease.
Lifestyle modifications to try to reverse the disease process itself is the most cost-effective and safe treatment for most cases of CVD. Medications play an important role; however, they can be a significant cause of patients’ morbidity and mortality.28 In comparison, treating the obesity epidemic, for example, would have a significant population-level effect and is much less cost-intensive.29
In an interesting meta-analysis, researchers compared the relative risk reduction with lifestyle changes to the typical medications prescribed to patients with coronary artery disease. The estimated reduction was 35% with smoking cessation, 25% with increased physical activity, and 45% with dietary changes.30 This is in comparison to reductions of 18% with low-dose aspirin use, 21% with statin use, 23% with beta-blocker use, and 26% with angiotensin-converting enzyme inhibitor use. This is not to say that providers should use lifestyle modification in isolation, but to demonstrate its effectiveness and highlight the potentially complimentary, additive, or even synergistic effect of combined lifestyle modification with optimal medical therapy.
The AHA and the American College of Cardiology (ACC) have launched initiatives promoting and educating both patients and physicians in lifestyle medicine. The ACC has demonstrated its commitment through an ongoing series called “CV Health Promotion”and recently dedicated an issue of the Journal of the American College of Cardiology to this topic.31 The AHA issued a call to action to effect behavior change. It published detailed recommendations on how to assess and intervene on behalf of patients by using a system called the “5 A’s”: assess unhealthy behavior, advise the patient how to change, agree through a shared process on the goals, assist with treatment, and arrange for follow-up and accountability.32
Cardiovascular Risk Scoring Systems
Well-established risk factors for CVD include age, male gender, smoking, diabetes, high blood pressure, high cholesterol, and early or strong family history of coronary artery disease. Of these, age and gender are not modifiable. These affect risk in proportion to their values, except for gender. Thus, making any change in blood pressure, lipids, or diabetes control is helpful, or in the case of worsening control, detrimental to health. These classic risk factors have formed the basis of the Framingham Risk Score. (See Table 2.)
Table 2. Classic and New Risk Factors or Metrics (Therapeutic Targets) |
|||
Classic or Traditional Risk Factors |
New Objective Risk Factors or Metrics |
New Subjective Risk Factors or Metrics |
Environmental Risk Factors |
|
|
|
|
The major determinants of cardiovascular risk remain lifestyle-mediated rather than genetic. Newer risk scores have improved the predictability of CVD risk by accounting for lifestyle components. Over time, several multivariate risk models have been developed to estimate CVD risk among healthy and asymptomatic individuals. The choice of a CVD calculator to estimate CVD risk score is determined by an individual’s characteristics, such as age, gender, and ethnicity.
Commonly used CVD risk scores in clinical practice include the Reynolds Risk Score and ACC/AHA pooled cohort equations with recent update (2018). The Reynolds Risk Score is distinctive because it incorporates premature family history of CAD and C-reactive protein (CRP) as variables. However, it does not include diabetes mellitus.33 Meanwhile, the ACC/AHA calculator does include diabetes mellitus but does not include family history of CAD; however, there might be a limitation in the applicability of this calculator for the general population.34
Factors such as obesity (BMI), waist circumference, body composition, physical activity, fitness level, type of diet, stress, quality of sleep, and environmental factors (noise and particulate pollution) have been identified as most likely driving classic CVD risk. Like traditional risk factors, these “lifestyle” risk factors also are potential therapeutic targets.
The current AHA initiative “Life’s Essential 8” (LE8) includes lifestyle key measures for improving and maintaining cardiovascular health. Previously known as LS7, this was updated to LE8 after sleep was included as one of its metrics. The LE8 metrics encompass health behaviors (diet, physical activity, nicotine exposure, and sleep) as well as health factors (BMI, blood lipids, blood glucose, and BP). Psychological health and well-being have the potential for preserving and improving cardiovascular health, but they were not included in LE8 as formal metrics because of their multidimensionality.35 Previous studies based on the LS7 reveal that meeting the goals for five to seven metrics was associated with a 72% reduction in CVD events, while meeting three to four metrics was associated with a 47% reduction in events.36
Several new analyses have helped us better understand the respective roles of individual risk factors. Using populational attributable risk, the INTERHEART study was able to determine the degree of effect that certain risk factors will have on the development of CVD. Further studies, such as PURE, have evaluated the effect of modifiable risk factors for CVD at a global level among multiple economic levels. They found that more than 70% of CVD cases were attributed to modifiable risk factors and that the largest populational attributable fraction was the result of metabolic factors (41.2%).37
Lifestyle change also is effective in reducing CVD risk among high-risk people with diabetes. Behavior changes reduced cardiovascular incidence by 52% and mortality by 68% in patients with diabetes.38 More importantly, healthy lifestyle (measured by cholesterol levels, BP, diet, smoking status, physical activity, and BMI), in a dose-dependent fashion, could reduce the risk of developing type 2 diabetes by up to 80%, showing the powerful preventive effect of lifestyle modification.39
Machine learning (ML) is providing new methods for risk scoring using the same nine CVD risk factors (age, sex, ethnicity, total cholesterol, high-density lipoprotein [HDL] cholesterol, systolic BP, treatment for hypertension, diabetes mellitus, and smoking). This specific study was based on Multi-Ethnic Study of Atherosclerosis (MESA) data and developed an ML risk calculator that reached a higher accuracy than the ACC/AHA risk calculator. Using identical data, they detected 13% more high-risk individuals as well identified 25% less unnecessary statin therapy in low-risk individuals. Currently further studies are underway to validate these findings.40
Another study presented the use of ML to identify Progression of Early Subclinical Atherosclerosis (EN-PESA) using age, systolic BP, dietary intake values, and common blood/urine tests to identify asymptomatic individuals with an increased risk of CVD. The results showed that EN-PESA performed better than atherosclerotic CVD and SCORE risk scores.41
Therapeutic Targets of Established Risk Factors
The Hard Targets: Weight, BMI, Waist Circumference, and Percent Body Fat
Obesity has increased gradually in the United States and nearly tripled since 1975 worldwide, according to the World Health Organization (WHO). Obesity rates have climbed from a crude prevalence of 37.9% in 2013-2014 to 39.8% in 2015-2016.42 It is associated directly with the cardiovascular risk factors of dyslipidemia, type 2 diabetes mellitus, hypertension, and sleep disorders. Obesity is an independent risk factor for cardiovascular disease mortality.43 Being 40 pounds over goal weight is one definition of obesity. However, frequent weight fluctuations, such as with yo-yo dieting, can negatively affect health. As little as a 3.88-pound (1.76 kg) increase in weight was associated with a 64% increased risk of any coronary event, an 85% higher risk of any CVD event, and a surprising 124% increased risk of death.44
A BMI of > 25 kg/m2 is considered overweight, while a BMI of > 30 kg/m2 is obese. Professional athletes commonly are included in the obese category because of their heavier weights, but they typically have low body fat and should not be classified as such. Although BMI is the most common method used to assess obesity and overweight, research showed that it is an insufficient metric in predicting body fat percentage.45 A recent study of National Football League athletes found an obesity rate of 53.4%, based on BMI. When graded by percentage of body fat, the obesity rate dropped to 8.9%.46 A population for whom BMI may become particularly helpful is children. By measuring a patient’s BMI trajectory, researchers were able to predict by 6 years of age which children would be obese as adolescents, thus, perhaps, allowing doctors and parents to screen high-risk children and intervene as early as possible.
A simple, fairly reproducible measurement is a waist circumference measurement. An indicator of body composition, specifically abdominal body fat, it is part of diagnosing metabolic syndrome, but it also is independently related to mortality.47,48 To be at risk based on waist circumference, measurements have to be > 40 inches (94 cm) in men and > 35 inches (80 cm) in women.49
The NHANES report from 1999-2016 showed an increase in weight, BMI, and waist circumference.27 Height did not change. For men, the mean weight has increased from 189.4 pounds to 197.9 pounds. The mean weight for women went up by 6.8 pounds. The mean waist circumference increased to 40.2 inches (102.1 cm) in men and to 38.6 in (98.0 cm) in women. Similarly, BMI has increased for both men and women. The mean BMI now is 29.1 kg/m2 in men and 29.6 kg/m2 in women.50
A better way to risk stratify patients is body composition, which can be measured by looking at percent body fat or lean body mass. Measuring body fat is becoming more important for several reasons. Weight loss has been the traditional way to measure improvement in health, but with the increased focus on exercise, and especially resistance training, it has become more important to track changes in body composition, since muscle is denser than fat. For men, a percent body fat of 18% to 25% is normal, > 26% is overweight, and > 38% is obese. For women, 25% to 31% is normal, > 32% is overweight, and > 42% is obese.
Muscle mass may be more important than the degree of fat. Grouped by high or low muscle and high or low fat, there was almost a 20% reduction in mortality in the two groups with high muscle mass vs. those with low muscle mass regardless of percent body fat content.51
Making direct measurements has become even more important because of two new phenomena. The first is the increase in the weight of the U.S. population, leading to a change in what is perceived as normal. When photos of overweight or obese children are shown to other children or mothers, they often are rated in the next lower category. Obese children often are rated as overweight, and overweight children often are graded as normal.52 This is caused by a drift or normalization of body size and weight as the result of the change in our population. Also, there is the new concept of TOFI — thin on the outside, fat on the inside — in which people have normal BMI but increased body fat.53 Physicians no longer can rely on the eyeball test or on patients’ stated metrics.
The Soft Target: Diet
Using food as medicine has been borne out in numerous studies showing the fundamental effect of diet on not only risk factor development, but also on overall event rates and even on mortality. Metrics such as BP, LDL, weight, waist circumference, BMI, and HbA1c can be measured easily and accurately. However, it is harder to measure dietary intake, since most surveys rely on patient recall, which allows for error and bias. An editorial called for the exclusion of dietary survey data in the medical literature, since it was not of high enough scientific quality.54 The results of multiple studies have been impressively uniform even though they are only observational and lower in quality because of their collection methods.
Researchers have studied (and continue to study) diet extensively, mostly in observational trials. One of the most important and interesting studies was the Mr-FIT study regarding Japanese migration.55 The investigators tracked Japanese patients in Japan, Hawaii, and San Francisco. When those of Japanese descent migrated from Japan to Hawaii to San Francisco, their CVD event rates doubled and their lipid levels increased similarly. BP did not follow this same pattern. Furthermore, at that time, smoking was nearly universal in the Japanese culture, so the change in event rates would best be explained by changes in lipids, which are closely associated with dietary changes.
Currently, the healthiest cardiovascular subpopulation is the Tsimané tribe in Bolivia, South America. They have the lowest degree of computed tomography (CT) calcium scoring ever recorded for a subgroup.56 Eighty-five percent of the population had a coronary calcium score of 0. Only 3% had a score higher than 100. They have almost no typical risk factors for CVD, and almost no clinical CVD events exist in their tribe, despite members eating 70% carbohydrates and having a high inflammatory burden (measured by elevated high-sensitivity C-reactive protein levels in 51% of the population).
The tribe is very active, eats mostly whole foods, does not smoke, and typically has normal BMIs. It will be interesting to see how their tribe is affected by the modern world.
In comparison, Americans eat a high-carbohydrate diet with the Standard American Diet (SAD) consisting mostly of highly processed and high-sugar foods.57 The PURE study investigators demonstrated that a high-carbohydrate diet was associated with a 28% increased rate of overall mortality compared to a diet with higher fat consumption.58 Interestingly, CVD mortality and events were not higher in the higher-carbohydrate group.
Authors of another study demonstrated the relative contribution of different dietary habits on mortality in the United States.59 Unlike the PURE study, which focused primarily on macronutrients, this study looked at subclasses of food (sodium intake, nuts, processed meats, seafood, vegetables, fruits, high-sugar beverages, whole grains, and red meat). The longitudinal nature of this study stands out because that allowed the investigators to track the changing U.S. dietary patterns. During the study, both sodium and red meat intake increased. Conversely, nut, whole grain, and fruit intake all declined. An encouraging finding was that sugar-sweetened beverages decreased almost 15%.
A good starting point to try to change dietary patterns and help build a balanced diet is the Harvard Healthy Eating Plate, which was developed on evidence-based data and has some significant differences from the U.S. Department of Agriculture MyPlate.60 Of note, both MyPlate and the Harvard Healthy Eating Plate recommend that half of one’s plate include fruits and vegetables.
Over time, there has been more evidence that increased servings of fruits and vegetables confer protection from heart disease and cancer. Authors of a recent study found an increasing incremental benefit of up to 10 servings per day.61 The threshold to achieve any risk reduction was only 2.5 servings per day, or less than one serving per meal. This large meta-analysis of more than 95 studies involving more than 2 million patients showed that an intake of 800 g/day of fruit and vegetables reduces the relative risk by 24% in heart disease, 33% in stroke, 13% in total cancer, and 31% in all-cause mortality.
The PURE healthy diet score is a scoring system for diet quality.62 The score uses seven foods that were linked with survival — fruits, vegetables, nuts, legumes, dairy, red meat, and fish. Scores range from 1 to 5 in all seven categories, with a total score of 7 to 35. The best groups were eight servings of fruits/vegetables per day, 2.5 servings of legumes and nuts per day, three servings of full-fat dairy per day, 1.5 servings of unprocessed meat per week, and two servings of fish per week. When comparing the healthiest scored diets to those of the lowest group, there was a significant effect on mortality and cardiovascular endpoints. When the score was applied to several large trials, researchers noted that diet was associated with a 24% reduction in mortality in the ONTARGET and TRANSCEND studies, a 22% reduction in mortality in the INTERHEART study, and a 25% reduction in stroke in the INTERSTROKE study.63-66
Vegetarian Diet
A vegetarian diet can have a similar effect on LDL as low-intensity statin therapy. Adhering to a completely vegetarian diet resulted in a 30% reduction of LDL in four weeks.67 This was similar to what was achieved with a low-intensity statin treatment over the same time.
However, a vegetarian or vegan diet is not necessarily a healthy diet. A recent study grading diet quality found that an unhealthy plant-based diet afforded the same risks as animal-based diets.68 The type of diet, per se, may not be as important as the actual elements being consumed.
Although it is outside the scope of this review to discuss different diet strategies, data from a well-done review article showed consistent elements between low-carb, low-fat/vegetarian/vegan, low-glycemic, Mediterranean, Paleolithic, and mixed/balanced diets. These included limited refined starches, added sugars, and processed foods; limited intake of certain fats; and increased intake of whole plant foods.69
Nuts and Fiber
The authors of several large studies found that nut intake of any kind, not just walnuts (which the AHA has supported for years), reduces mortality.70,71 Daily nut intake was associated with a 20% relative risk reduction. These studies did not differentiate between types of nuts or even salted vs. non-salted nuts. The intake of any type of nuts was found to be protective. A concern regarding nut intake is that nuts are calorie-dense and could lead to weight gain. However, moderate consumption can mitigate this concern.
Fiber has been recommended for risk reduction of overall mortality, CVD, type 2 diabetes, and colon cancer. The current recommendation is at least 25 g of fiber per day. In a large meta-analysis, investigators demonstrated a 15% to 30% reduction in the previously mentioned outcomes when comparing the highest to the lowest amount of consumed fiber.72
The Importance of Breakfast
In a sub-study of the PESA trial, investigators analyzed the importance of eating breakfast.73 Although they found that eating breakfast was protective, they further divided the groups into eating clusters: a Mediterranean eating cluster, a Western eating cluster, and a social business eating cluster.
The social eating cluster skipped breakfast most often and snacked the most, likely correlating with a busy schedule, rushed eating, and eating on the go. Not surprisingly, this group also had the worst outcomes, thus pointing to the possibility that a busy lifestyle and eating fast food, rather than skipping breakfast, actually is the more problematic habit.
Sugar Intake
Sugar intake has been directly associated with mortality, with a four-fold increase in mortality between the lowest and the highest sugar consumption. The highest sugar consumers obtained more than 30% of their calories from sugar.74 The largest contributor of excess sugar identified was sweetened beverages, including soda, tea, energy drinks, and juices. Researchers estimated the number of excess deaths in countries attributed to soda consumption. Mexico had the highest number of attributable deaths to soda, with 30% of the risk of death being attributable to soda. The United States was in fourth place.75
Worldwide, the model estimated that soda contributed to approximately 184,000 deaths annually. Deaths from sugar-sweetened beverages were predicted to outpace violent deaths in Mexico. A strategy of reducing exposure to these products and drinking water instead could have a substantial effect on populational health.
Many suggest that sugar-free drinks may not be harmful because of the lack of refined sugar. In direct opposition to this notion, researchers have found an almost 300% increase in stroke and dementia from consuming diet soda.76 Moreover, in another study looking at the gut biome, investigators found that about one in five people have a gut flora pattern that made patients who ingested artificial sweeteners more susceptible to diabetes even though they were not ingesting real sugar.77
Meat Consumption
There is growing evidence that meat intake inversely affects mortality. One daily serving of red meat can increase mortality by 13%, while processed meats can increase it by 20%.78 When meat was replaced by another protein source, such as beans, whole grains, or nuts, mortality was reduced by 10%, 14%, and 19%, respectively.
Further supporting these observational data are several studies demonstrating how meat can lead to increased cardiovascular events and mortality. Two important studies demonstrated that when L-carnitine, a nutrient found in red meat, is processed by normal gut flora, it produces trimethylamine N-oxide (TMAO), which leads to platelet hyperreactivity and promotes atherosclerosis.79,80 Other mechanisms identified were heme iron and nitrates. This may explain why red meat is associated with cardiovascular disease more strongly than white meat.81
Several studies proved the health benefits of the Dietary Approaches to Stop Hypertension (DASH) diet. These benefits include lowering high blood pressure, improving dyslipidemia, and reducing the risk of diabetes and CVD.82-84 The DASH diet recommends eating vegetables, fruits, whole grains, and fat-free and low-fat dairy products while limiting foods that are high in saturated fat, such as fatty meats, full-fat dairy products, and sugar-sweetened beverages.
The Mediterranean diet, which is based on consuming extra virgin olive oil, fruits and vegetables, fish, nuts, and limited amounts of red meat, has been found to reduce mortality by about 30%.85 Using a risk score based on compliance with a Mediterranean diet, researchers found that, as patients ate more of the recommended foods, CVD event rates were reduced.86
For every one-point increase in diet score, there was a 5% reduction in event rates. There was a 3.5% absolute risk reduction when comparing the highest to the lowest diet scores. This gives a number needed to treat (NNT) of only 28 patients to avoid one major CVD event. The authors noted that a better strategy may be to focus on recommending that people eat more of the good food items rather than focusing on what foods to avoid.
A final concern about eating healthy is the cost. Although many believe eating healthy is cost-prohibitive, investigators showed that the cost of healthy, isocaloric foods averages out to only $1.50 more per day per person.87 This may not be extrapolated well to organic foods or to situations such as food deserts, where healthy food is not an option.
The Soft to Hard Target: Physical Activity
The current Physical Activity Guidelines for Americans recommendations are for 150 to 300 minutes of moderate-intensity physical activity per week, 75 to 150 minutes of vigorous-intensity aerobic physical activity per week, or a combination that averages out to 25 to 50 minutes per day or 12.5 to 25 minutes per day, respectively (assuming six days of activity per week).88 Moderate exercise can be achieved by heavy yard work, brisk walking, water aerobics, or swimming laps. It is recommended to start with one or two goals of frequency, intensity, and duration, with increments of physical activity as tolerated.
However, only approximately 20% of adults meet the key guidelines for physical activity. Meeting the guidelines can reduce up to 33% of all-cause mortality. On the contrary, insufficient physical activity is related to an estimated cost of $117 billion per year and 10% of premature mortality.
Furthermore, a link between sitting time and all-cause and CVD mortality risk among adults has been established. A study of 222,497 adults in Australia found a consistent increased risk for all-cause mortality beyond age, sex, and BMI index and independent of physical activity.89
Nonetheless, research that looked into the stratified association of intensity of physical activity and reduction in mortality found that replacing sedentary behavior with light activity for 30 minutes led to a 17% reduction in mortality, while moderate to vigorous exercise was associated with a 35% reduction in mortality.90 To benefit from the mortality reduction, the patient had to reduce (replace) sedentary time with physical activity, not simply increase exercise time.
Although most people believe that the diabetes and obesity epidemics mostly have been driven by excess calories, some data point toward lack of exercise as a strong contributing factor. The percentage of people who now perform no leisure-time physical activity has doubled from 1988 to 2010.91 Physical activity also has an epigenetic effect on obesity development. In two subgroups of patients who were genetically predisposed to developing obesity, physical activity modified the development of obesity by up to 40%.92
Exercise and obesity are not always related or causal. Researchers found that both physical activity and obesity have their own relative contribution to mortality and, furthermore, that physical activity was more protective than being at an ideal weight. Physical activity reduces the risk of death by 7.35% compared to non-obesity, which reduced death by 3.66%, a two-fold difference in effect.93
Physical activity as a factor to decrease mortality is well established. The earliest examples come from the cardiac rehabilitation literature, which showed that supervised physical activity early after MI led to reduced mortality. In a large study in Sweden, investigators demonstrated that, compared to post-MI survivors who were not active, those who were active consistently over the next year had a 71% risk reduction in mortality. Even subjects who did less physical activity (reduced activity group) had a 44% reduction, while those who started late (increased activity group) showed an intermediate 59% reduction.94
In a large meta-analysis that included 391 trials, exercise had a similar BP-lowering effect as most single pharmacologic agents (-2.9 mmHg to -5.0 mmHg). This held true for both endurance and resistance types of exercise.95 We can infer that physical activity can provide similar effectiveness as standard blood pressure medications.
In the CLEVER trial, a small study comparing optimal medical therapy vs. stenting vs. physical activity for treatment of claudication among patients with aortoiliac peripheral artery disease (PAD), researchers found that physical activity led to the greatest increase in walking distance. The caveat in this study was that the physical activity was supervised exercise therapy and was not patient reported.96
The level of physical activity needed to affect mortality has been studied extensively. In a large-scale study from Taiwan, researchers showed that not only duration but also intensity factored into mortality reduction.97
Performing 15 minutes of continuous, moderate exercise was enough to start separating the survival curves, although intense exercise had an earlier effect. Even 10 minutes of continuous jogging (albeit at a 10-minutes-per-mile pace) can reduce mortality; however, increased exercise volume and intensity can further reduce mortality.98
Physical Activity and Mortality
There are only a few studies that have shown a U-shaped relationship between physical activity and mortality. The most famous is the Copenhagen Heart Study, which demonstrated that both the low physical activity group and the vigorous physical activity group had the highest mortality.
Conversely, there was a progressive decline in mortality from the lowest to the mild to the moderate groups, ultimately reversing the mortality trend with the more vigorous group.99 The highest physical activity group in this study had relatively high event rates, but since that group was the smallest sample size (36 total patients), this could represent a type II beta error (false-positive). A later study, which included more than 200,000 patients total and more than 57,000 patients in the vigorous group, found the expected incremental decrease in mortality with increased physical activity.100
Previous studies of endurance events, such as marathon running, have been associated with a risk of death during the activity.101 Nonetheless, several factors should be noted. The overall event rate was low, at 0.67 per 100,000 persons. During the 10 years of follow-up, there were only 59 cardiac arrests. Further, a large meta-analysis of running studies estimated that runners live three years longer than non-runners, and every hour of running added seven hours to the lifespan.102
Patients often inquired regarding short bursts of intermittent physical activity: Could this be deleterious to health? Researchers demonstrated that such “weekend warriors” actually benefited from less-than-optimal physical activity vs. non-physical activity. Although regularly active men had a 37% reduction in mortality, intermittent weekend warriors still had a 22% reduction in mortality.103
Being active and staying active results in the lowest mortality rate among people with CVD and, as expected, being inactive and staying inactive has the highest mortality. This was demonstrated in a study where active patients who became inactive had the second highest cardiovascular mortality, although inactive patients who became active were the same as the active-active group.104 Physical activity is a unique “magic pill” to help patients live longer and be healthier.
Watching television can harm patients acutely and in longevity. A study showed that every one hour of television watching increased overall mortality by 11% and CVD mortality by 18%.105
Data Reporting
Most physical activity data are self-reported survey data; however, with the advent of wearables that measure steps, distance, and calories burned, there has been increased data regarding the number of steps needed for optimal health. A large, worldwide study of more than 700,000 patients in 111 countries found the daily average steps to be 4,961.
In the United States, the average steps were fewer, at 4,774. Step count also correlated with national obesity rates, but a stronger correlation was found in activity inequality, which was a measure of the variation in steps across the population of a country. The wider the activity inequality, the higher the obesity rate. In terms of this metric, the United States was the fourth worst country studied. Of interest, the researchers noted the activity inequality metric mostly was the result of reduced steps in women.106
Cardiorespiratory Fitness
Cardiorespiratory fitness (CRF) is a component of physiologic fitness related to the ability of respiratory and circulatory systems to supply oxygen during sustained physical activity. Several studies demonstrated a relationship between CRF and decreased all-cause mortality and CVD mortality.107,108 The authors of a study on CRF, self-reported physical activity, and grip strength found that increases in any and/or all of these three areas equated to a reduced degree of developing CVD. The strongest trends were seen in both measured variables, with the weakest trend being self-reported physical activity.109
Measured CRF in middle age can predict not only CVD, but also overall mortality. Furthermore, early adulthood and midlife CRF has been associated with lower premature death and CVD events.110 Another study found significant differences in overall, cardiovascular, and cancer mortality when measuring CRF.111 For each increase in MET (metabolic equivalent) level, there was an 11.6%, 16.1%, and 14.0% reduction in all-cause, cardiovascular, and cancer mortality, respectively. In this study, the least fit group had a 73% increase in all-cause mortality and doubled cancer mortality when compared to the most fit group.
Changes in CRF also are important, since one can change their risk profile by becoming more fit through exercise. In a study with more than 23 years of follow-up, researchers used two separate bicycle stress tests to assess fitness in a group of healthy, middle-aged men.112 The group with the highest event rate was the “became unfit” group. Even those with high fitness at the start of the study had a 235% increase in risk of stroke and a 174% increase in risk of death if they became unfit. In contrast, those with the lowest fitness had a 60% reduction in stroke risk and a 34% reduction in death if they moved into the “became fit” group.
A cardiovascular exercise program to help individuals with CVD should be more commonplace among clinicians as they continue to understand the benefits of physical activity to prevent and treat CVD. Investigators demonstrated that increased fitness levels (able to do 10 METs) significantly attenuated patients’ 30-year CVD mortality risk across all groups of risk factor distribution.113 Obtaining a standard treadmill test for exercise prescription may become more commonplace, since the population is getting less and less active and people tend to overestimate their level of physical activity. Treadmill tests also can be used to screen for CVD, measure the safety of starting an exercise program, determine prognosis, and, finally, set heart rate target goals.
Emerging Risk Factors
Climate Change and CVD
Progressive climate change and individual environmental exposure have been closely related with cardiovascular health. Certain communities may have less capacity to cope with these changes and, therefore, are more sensitive to their effects. In particular, older adults, patients with preexisting CVD, and people with limited socioeconomical standing may be more vulnerable, thus resulting in worse health outcomes for those groups.114
Environmental factors and their interactions are increasingly more important in predicting hospitalizations as the result of acute cardiovascular events as a patient ages. A recent population study in Canada on “Weather, Air Pollution, and Acute Cardiac Hospitalizations” modeled the association between multiple environmental factors (air pressure, temperature, wind speed, precipitation, and air pollutants) and acute cardiovascular events stratified by age. For example, heart failure in older patients was associated with low-pressure systems, low temperatures, both high and low wind speeds, wet conditions, and air pollutants (carbon monoxide, sulfur dioxide, ozone, and fine particulate matter [PM2.5]). These associations can become clinically relevant in providing patients with educational materials and resources to potentially reduce exacerbations through recognizing and mitigating these environmental risk factors.115
Air Pollution and CVD
A short- and long-term exposure to PM2.5 has been linked to an increase in cardiovascular mortality and was identified as an independent modifiable risk factor.116 As early as 2010, the AHA published information on the causal relationship between PM2.5 and CVD.117 A 10 mcg/m3 increase in long-term average PM2.5 exposure is associated with an approximately 10% increase in all-cause mortality.117 More recently, a 10 mcg/m3 exposure has been associated with an increased risk of ischemic heart disease mortality (23%), cerebrovascular mortality (24%), incident stroke (13%), and incident myocardial infarction (8%). The pathways through which PM2.5 exposure increases CVD risk primarily are oxidative stress and systemic inflammation.116,118 Other mechanisms identified are direct translocation into systemic circulation and perturbation of the autonomic system.116
Simple lifestyle changes can help limit air pollution exposure and CVD risk, especially in high-risk individuals. For example, avoidance of proximity to major roadways could help reduce exposure to traffic-derived pollutants, and staying indoors with appropriate air filtration in environments with high ambient PM2.5 also can help reduce exposure.119
Although air pollution is an independent risk factor, it should not reduce a low-risk patient’s opportunities to exercise. An American Medical Association statement noted that the benefits of aerobic exercise nearly always exceed the risk of air pollution exposure across a range of concentrations and for long durations of exercise for healthy individuals.119
A study in 2019 with more than 500,000 people in the United States identified a Mediterranean diet as reducing CVD risk related to long-term PM2.5 exposure.120 Further clinical action guidelines and, even more importantly, national and international health policies are especially needed to prevent and mitigate air pollution effects on CVD risk.121
Sleep and CVD
Thirty-four percent of Americans do not get the recommended seven hours of sleep per night.122 In a consensus statement after reviewing 5,314 scientific articles, the American Academy of Sleep Medicine and the Sleep Research Society concluded that fewer than seven hours of sleep per night is associated with weight gain, obesity, diabetes, hypertension, heart disease, stroke, depression, and an increased risk of mortality.123 Short sleep also was associated with worse immune function, increased error rate, and increased accidents. Emerging evidence suggests that increasing sleep duration benefits cardiovascular health.124 Short sleep duration may be a causal risk factor for CAD, while an increase in sleep duration is protective.124 This brings us to the question of whether extending sleep duration might be a strategy for reducing CVD risk, especially in short sleepers.
Short sleep can have an additive effect on cardiac risk factors, leading to death from heart disease, stroke, and cancer.125 In a cohort of 1,654 subjects, less than six hours of sleep was associated with an increased mortality. The limitation of this study was that there was only a single determination of sleep duration; however, this study was particularly interesting since sleep duration was measured in a sleep lab instead of being self-reported, making this a much more objective measure of sleep. Further education and emphasis regarding sleep care and management of chronic sleep disorders are important for the overall prevention of CVD.
Summary
CVD is the leading cause of premature morbidity and mortality in the United States and worldwide. It has a serious effect on patients’ quality of life. The risk factors driving the rates of CVD are well known, and it is clear that lifestyle decisions drive the risk factors. Providers should recommend initiating lifestyle interventions with an individually tailored program that simultaneously addresses multiple risk factors and lifestyle habits. Lifestyle modification represents a highly effective and low-cost intervention that works synergistically with pharmacotherapy to reduce the incidence, progression, and mortality associated with CVD.
References
- Xu J, Murphy SL, Kochanek KD, Arias E. Mortality in the United States, 2021. Key findings: Data from the National Vital Statistics System. Published December 2022. https://www.cdc.gov/nchs/products/databriefs/db456.htm#:~:text=Life%20expectancy%20for%20the%20U.S.,group%201%20year%20and%20over
- Dagenais GR, Leong DP, Rangarajan S, et al. Variations in common diseases, hospital admissions, and deaths in middle-aged adults in 21 countries from five continents (PURE): A prospective cohort study. Lancet 2020;395:785-794.
- Mensah GA, Wei GS, Sorlie PD, et al. Decline in cardiovascular mortality: Possible causes and implications. Circ Res 2017;120:366-380.
- Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2019;74:1376-1414.
- Khera AV, Emdin CA, Drake I, et al. Genetic risk, adherence to a healthy lifestyle, and coronary disease. N Engl J Med 2016;375:2349-2358.
- Ruby JG, Wright KM, Rand KA, et al. Estimates of the heritability of human longevity are substantially inflated due to assortative mating. Genetics 2018;210:1109-1124.
- Li Y, Pan A, Wang DD, et al. Impact of healthy lifestyle factors on life expectancies in the US population. Circulation 2018;138:345-355.
- Taler SJ. Initial treatment of hypertension. N Engl J Med 2018;378:636-644.
- Centers for Disease Control and Prevention. Facts about hypertension. Last reviewed July 6, 2023. https://www.cdc.gov/bloodpressure/facts.htm
- Merai R, Siegel C, Rakotz M, et al. CDC Grand Rounds: A public health approach to detect and control hypertension. MMWR Morb Mortal Wkly Rep 2016;65:1261-1264.
- Centers for Disease Control and Prevention. Prevalence of both diagnosed and undiagnosed diabetes. National Diabetes Statistics Report. Last reviewed Sept. 30, 2022. https://www.cdc.gov/diabetes/data/statistics-report/diagnosed-undiagnosed-diabetes.html
- Mercado C, DeSimone AK, Odom E, et al. Prevalence of cholesterol treatment eligibility and medication use among adults — United States, 2005-2012. MMWR Morb Mortal Wkly Rep 2015;64:1305-1311.
- Temple NJ. The origins of the obesity epidemic in the USA – lessons for today. Nutrients 2022;14:4253.
- Wilding JPH, Batterham RL, Davies M, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension. Diabetes Obes Metab 2022;24:1553-1564.
- Yanovski SZ, Yanovski JA. Long-term drug treatment for obesity: A systematic and clinical review. JAMA 2014;311:74-86.
- Rajagopalan S, Brauer M, Bhatnagar A, et al. Personal-level protective actions against particulate matter air pollution exposure: A scientific statement from the American Heart Association. Circulation 2020;142:e411-e431.
- Colantonio LD, Rosenson RS, Deng L, et al. Adherence to statin therapy among US adults between 2007 and 2014. J Am Heart Assoc 2019;8:e010376.
- Rodriguez F, Maron DJ, Knowles JW, et al. Association of statin adherence with mortality in patients with atherosclerotic cardiovascular disease. JAMA Cardiol 2019;4:206-213.
- Dusetzina SB, Besaw RJ, Whitmore CC, et al. Cost-related medication nonadherence and desire for medication cost information among adults aged 65 years and older in the US in 2022. JAMA Netw Open 2023;6:e2314211.
- Wang TY, Kaltenbach LA, Cannon CP, et al. Effect of medication co-payment vouchers on P2Y12 inhibitor use and major adverse cardiovascular events among patients with myocardial infarction. JAMA 2019;321:44-55.
- Farkouh ME, Boden WE, Bittner V, et al. Risk factor control for coronary artery disease secondary prevention in large randomized trials. J Am Coll Cardiol 2013;61:1607-1615.
- Brown TM, Voeks JH, Bittner V, et al. Achievement of optimal medical therapy goals for U.S. adults with coronary artery disease: Results from the REGARDS Study (Reasons for Geographic And Racial Differences in Stroke). J Am Coll Cardiol 2014;63:1626-1633.
- Yang Q, Cogswell ME, Flanders WD, et al. Trends in cardiovascular health metrics and associations with all-cause and CVD mortality among US adults. JAMA 2012;307:1273-1283.
- GBD 2016 Lifetime Risk of Stroke Collaborators; Feigin VL, Nguyen G, Cercy K, et al. Global, regional, and country-specific lifetime risks of stroke, 1990 and 2016. N Engl J Med 2018;379:2429-2437.
- Teo K, Lear S, Islam S, et al. Prevalence of a healthy lifestyle among individuals with cardiovascular disease in high-, middle- and low-income countries: The Prospective Urban Rural Epidemiology (PURE) study. JAMA 2013;309:1613-1621.
- Devries S, Agatston A, Aggarwal M, et al. A deficiency of nutrition education and practice in cardiology. Am J Med 2017;130:1298-1305.
- Grabovac I, Smith L, Stefanac S, et al. Health care providers’ advice on lifestyle modification in the US population: Results from the NHANES 2011-2016. Am J Med 2019;132:489-497.e1.
- Budnitz DS, Lovegrove MC, Shehab N, Richards CL. Emergency hospitalizations for adverse drug events in older Americans. N Engl J Med 2011;365:2002-2012.
- Yusuf S, Pitt B. A lifetime of prevention: The case of heart failure. Circulation 2002;106:2997-2998.
- Iestra JA, Kromhout D, van der Schouw YT, et al. Effect size estimates of lifestyle and dietary changes on all-cause mortality in coronary artery disease patients. Circulation 2005;112:924-934.
- Turco JV, Inal-Veith A, Fuster V. Cardiovascular health promotion: An issue that can no longer wait. J Am Coll Cardiol 2018;72:908-913.
- Spring B, Ockene JK, Gidding SS, et al. Better population health through behavior change in adults: A call to action. Circulation 2013;128:2169-2176.33.
- Ridker PM, Buring JE, Rifai N, Cook NR. Development and validation of improved algorithms for the assessment of global cardiovascular risk in women: The Reynolds RISK Score. JAMA 2007;297:611-619.
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019;139:e1082-e1143.
- Lloyd-Jones DM, Allen NB, Anderson CAM, et al. Life’s Essential 8: Updating and enhancing the American Heart Association’s construct of cardiovascular health: A presidential advisory from the American Heart Association. Circulation 2022;146:e18-e43.
- Ramírez-Vélez R, Saavedra JM, Lobelo F, et al. Ideal cardiovascular health and incident cardiovascular disease among adults: A systematic review and meta-analysis. Mayo Clin Proc 2018;93:1589-1599.
- Yusuf S, Joseph P, Rangarajan S, et al. Modifiable risk factors, cardiovascular disease, and mortality in 155-722 individuals from 21 high-income, middle-income, and low-income countries (PURE): A prospective cohort study. Lancet 2020;395:795-808.
- Liu G, Li Y, Hu Y, et al. Influence of lifestyle on incident cardiovascular disease and mortality in patients with diabetes mellitus. J Am Coll Cardiol 2018;71:2867-2876.
- Joseph JJ, Bennett A, Echouffo Tcheugui JB, et al. Ideal cardiovascular health, glycaemic status and incident type 2 diabetes mellitus: The REasons for Geographic and Racial Differences in Stroke (REGARDS) study. Diabetologia 2019;62:426-437.
- Kakadiaris IA, Vrigkas M, Yen AA, et al. Machine learning outperforms ACC/AHA CVD risk calculator in MESA. J Am Heart Assoc 2018;7:e009476.
- Sánchez-Cabo F, Rossello X, Fuster V, et al. Machine learning improves cardiovascular risk definition for young, asymptomatic individuals. J Am Coll Cardiol 2020;76:1674-1685.
- Flegal KM, Kruszon-Moran D, Carroll MD, et al. Trends in obesity among adults in the United States, 2005 to 2014. JAMA 2016;315:2284-2291.
- Powell-Wiley TM, Poirier P, Burke LE, et al. Obesity and cardiovascular disease A scientific statement from the American Heart Association. Circulation 2021;143:e984-e1010.
- Bangalore S, Fayyad R, Laskey R, et al. Body-weight fluctuations and outcomes in coronary disease. N Engl J Med 2017;376:1332-1340.
- Pack QR, Rodriguez-Escudero JP, Thomas RJ, et al. Diagnostic performance of weight loss to predict body fatness improvement in cardiac rehabilitation patients. J Cardiopulm Rehabil Prev 2013;33:68-76.
- Provencher MT, Chahla J, Sanchez G, et al. Body mass index versus body fat percentage in prospective National Football League athletes: Overestimation of obesity rate in athletes at the National Football League scouting combine. J Strength Cond Res 2018;32:1013-1019.
- Sahakyan KR, Somers VK, Rodriguez-Escudero JP, et al. Normal-weight central obesity: Implications for total and cardiovascular mortality. Ann Intern Med 2015;163:827-835.
- Cerhan JR, Moore SC, Jacobs EJ, et al. A pooled analysis of waist circumference and mortality in 650,000 adults. Mayo Clin Proc 2014;89:335-345.
- Huang PL. A comprehensive definition for metabolic syndrome. Dis Model Mech 2009;2:231-237.
- Fryar CD, Kruszon-Moran D, Gu Q, Ogden CL. Mean body weight, height, waist circumference, and body mass index among adults: United States, 1999-2000 through 2015-2016. National Health Statistics Report. Published Dec. 20, 2018. https://www.cdc.gov/nchs/data/nhsr/nhsr122-508.pdf
- Srikanthan P, Horwich TB, Tseng CH. Relation of muscle mass and fat mass to cardiovascular disease mortality. Am J Cardiol 2016;117:1355-1360.
- Sarafrazi N, Hughes JP, Borrud L, et al. Perception of weight status in U.S. children and adolescents aged 8-15 years, 2005-2012. NCHS Data Brief. Published July 2014. http://www.cdc.gov/nchs/data/databriefs/db158_table.pdf#3
- Zdrojewicz Z, Popowicz E, Szyca M, et al. TOFI phenotype – its effect on the occurrence of diabetes. Pediatr Endocrinol Diabetes Metab 2017;23:96-100.
- Archer E, Pavela G, Lavie CJ. The inadmissibility of what we eat in America and NHANES dietary data in nutrition and obesity research and the scientific formulation of national dietary guidelines. Mayo Clin Proc 2015;90:911-926.
- Marmot MG, Syme SL, Kagan A, et al. Epidemiologic studies of coronary heart disease and stroke in Japanese men living in Japan, Hawaii and California: Prevalence of coronary and hypertensive heart disease and associated risk factors. Am J Epidemiol 1975;102:514-525.
- Kaplan H, Thompson RC, Trumble BC, et al. Coronary atherosclerosis in indigenous South American Tsimane: A cross-sectional cohort study. Lancet 2017;389:1730-1739.
- Grotto D, Zied E. The standard American diet and its relationship to the health status of Americans. Nutr Clin Pract 2010;25:603-612.
- Dehghan M, Mente A, Zhang X, et al. Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): A prospective cohort study. Lancet 2017;390:2050-2062.
- Micha R, Peñalvo JL, Cudhea F, et al. Association between dietary factors and mortality from heart disease, stroke, and type 2 diabetes in the United States. JAMA 2017;317:912-924.
- Harvard T.H. Chan School of Public Health. Healthy Eating Plate. https://www.hsph.harvard.edu/nutritionsource/healthy-eating-plate/
- Aune D, Giovannucci E, Boffetta P, et al. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality—a systematic review and dose-response meta-analysis of prospective studies. Int J Epidemiol 2017;46:1029-1056.
- Miller V, Mente A, Dehghan M, et al. Fruit, vegetable, and legume intake, and cardiovascular disease and deaths in 18 countries (PURE): A prospective cohort study. Lancet 2017;390:2037-2049.
- Yusuf S, Hawken S, Ôunpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004;364:937-952.
- ONTARGET Investigators; Yusuf S, Teo KK, Pogue J, et al. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med 2008;358:1547-1559.
- O’Donnell MJ, Chin SL, Rangarajan S, et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): A case-control study. Lancet 2016;388:761-775.
- Mente A. Higher healthy diet score: Reduced CV disease and mortality worldwide. Presented at the ESC congress, Munich, Germany, 2018. European Society of Cardiology. https://ipccs.org/2018/09/04/higher-healthy-diet-score-reduced-cv-disease-and-mortality-worldwide/
- Jenkins DJ, Kendall CW, Marchie A, et al. Direct comparison of a dietary portfolio of cholesterol-lowering foods with a statin in hypercholesterolemic participants. Am J Clin Nutr 2005;81:380-387.
- Satija A, Bhupathiraju SN, Spiegelman D, et al. Healthful and unhealthful plant-based diets and the risk of coronary heart disease in U.S. adults. J Am Coll Cardiol 2017;70:411-422.
- Katz DL, Meller S. Can we say what diet is best for health? Annu Rev Public Health 2014;35:83-103.
- Bao Y, Han J, Hu FB, et al. Association of nut consumption with total and cause-specific mortality. N Engl J Med 2013;369:2001-2011.
- Hu FB, Stampfer MJ, Manson JE, et al. Dietary fat intake and the risk of coronary heart disease in women. N Engl J Med 1997;337:1491-1499.
- Reynolds A, Mann J, Cummings J, et al. Carbohydrate quality and human health: A series of systematic reviews and meta-analyses. Lancet 2019;393:434-445.
- Uzhova I, Fuster V, Fernández-Ortiz A, et al. The importance of breakfast in atherosclerosis disease: Insights from the PESA study. J Am Coll Cardiol 2017;70:1833-1842.
- Yang Q, Zhang Z, Gregg EW, et al. Added sugar intake and cardiovascular diseases mortality among US adults. JAMA Intern Med 2014;174:516-524.
- Singh GM, Micha R, Khatibzadeh S, et al. Estimated global, regional, and national disease burdens related to sugar-sweetened beverage consumption in 2010. Circulation 2015;132:639-666.
- Pase MP, Himali JJ, Beiser AS, et al. Sugar- and artificially sweetened beverages and the risks of incident stroke and dementia. Stroke 2017;48:1139-1146.
- Suez J, Korem T, Zeevi D, et al. Artificial sweeteners induce glucose intolerance by altering the gut microbiota. Nature 2014;514:181-186.
- Pan A, Sun Q, Bernstein AM, et al. Red meat consumption and mortality: Results from 2 prospective cohort studies. Arch Intern Med 2012;172:555-563.
- Koeth RA, Wang Z, Levison BS, et al. Intestinal microbiota metabolism of L-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat Med 2013;19:576-585.
- Zhu W, Gregory JC, Org E, et al. Gut microbial metabolite TMAO enhances platelet hyperreactivity and thrombosis risk. Cell 2016;165:111-124.
- Etemadi A, Sinha R, Ward MH, et al. Mortality from different causes associated with meat, heme iron, nitrates, and nitrites in the NIH-AARP Diet and Health Study: Population based cohort study. BMJ 2017;357:j1957.
- Sacks FM, Svetkey LP, Vollmer WM, et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. N Engl J Med 2001;344:3-10.
- Conlin PR. The Dietary Approaches to Stop Hypertension (DASH) clinical trial: Implications for lifestyle modifications in the treatment of hypertensive patients. Cardiol Rev 1999;7:284-288.
- Moore TJ, Conlin PR, Ard J, Svetkey LP. DASH (Dietary Approaches to Stop Hypertension) diet is effective treatment for stage 1 isolated systolic hypertension. Hypertension 2001;38:155-158.
- Estruch R, Ros E, Salas-Salvadó J, et al. Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts. N Engl J Med 2018;378:e34.
- Stewart RAH, Wallentin L, Benatar J, et al. Dietary patterns and the risk of major adverse cardiovascular events in a global study of high-risk patients with stable coronary heart disease. Eur Heart J 2016;37:1993-2001.
- Rao M, Afshin A, Singh G, Mozaffarian D. Do healthier foods and diet patterns cost more than less healthy options? A systematic review and meta-analysis. BMJ Open 2013;3:e004277.
- Piercy KL, Troiano RP, Ballard RM, et al. The Physical Activity Guidelines for Americans. JAMA 2018;320:2020-2028.
- Van der Ploeg HP, Chey T, Korda RJ, et al. Sitting time and all-cause mortality risk in 222 497 Australian adults. Arch Intern Med 2012;172:494-500.
- Diaz KM, Duran AT, Colabianchi N, et al. Potential effects on mortality of replacing sedentary time with short sedentary bouts or physical activity: A national cohort study. Am J Epidemiol 2019;188:537-544.
- Ladabaum U, Mannalithara A, Myer PA, Singh G. Obesity, abdominal obesity, physical activity, and caloric intake in US adults: 1988 to 2010. Am J Med 2014;127:717-727.e12.
- Li S, Zhao JH, Luan J, et al. Physical activity attenuates the genetic predisposition to obesity in 20,000 men and women from EPIC-Norfolk prospective population study. PLoS Med 2010;7:e1000332.
- Ekelund U, Ward HA, Norat T, et al. Physical activity and all-cause mortality across levels of overall and abdominal adiposity in European men and women: The European Prospective Investigation into Cancer and Nutrition Study (EPIC). Am J Clin Nutr 2015;101:613-621.
- Ekblom O, Ek A, Cider Å, et al. Increased physical activity post-myocardial infarction is related to reduced mortality: Results from the SWEDEHEART Registry. J Am Heart Assoc 2018;7:e010108.
- Naci H, Salcher-Konrad M, Dias S, et al. How does exercise treatment compare with antihypertensive medications? A network meta-analysis of 391 randomised controlled trials assessing exercise and medication effects on systolic blood pressure. Br J Sports Med 2019;53:859-869.
- Murphy TP, Cutlip DE, Regensteiner JG, et al. Supervised exercise, stent revascularization, or medical therapy for claudication due to aortoiliac peripheral artery disease: The CLEVER study. J Am Coll Cardiol 2015;65:999-1009.
- Wen CP, Wai JPM, Tsai MK, et al. Minimum amount of physical activity for reduced mortality and extended life expectancy: A prospective cohort study. Lancet 2011;378:1244-1253.
- Stewart RAH, Held C, Hadziosmanovic N, et al. Physical activity and mortality in patients with stable coronary heart disease. J Am Coll Cardiol 2017;70:1689-1700.
- Schnohr P, O’Keefe JH, Marott JL, et al. Dose of jogging and long-term mortality. J Am Coll Cardiol 2015;65:411-419.
- Gebel K, Ding D, Chey T, et al. Effect of moderate to vigorous physical activity on all-cause mortality in middle-aged and older Australians. JAMA Intern Med 2015;175:970-977.
- Kim JH, Malhotra R, Chiampas G, et al. Cardiac arrest during long-distance running races. N Engl J Med 2012;366:130-140.
- Lee DC, Brellenthin AG, Thompson PD, et al. Running as a key lifestyle medicine for longevity. Prog Cardiovasc Dis 2017;60:45-55.
- O’Donovan G, Lee IM, Hamer M, Stamatakis E. Association of “weekend warrior” and other leisure time physical activity patterns with risks for all-cause, cardiovascular disease, and cancer mortality. JAMA Intern Med 2017;177:335-342.
- Lahtinen M, Toukola T, Junttila MJ, et al. Effect of changes in physical activity on risk for cardiac death in patients with coronary artery disease. Am J Cardiol 2018;121:143-148.
- Dunstan DW, Barr ELM, Healy GN, et al. Television viewing time and mortality: The Australian Diabetes, Obesity and Lifestyle Study (AusDiab). Circulation 2010;121:384-391.
- Althoff T, Sosič R, Hicks JL, et al. Large-scale physical activity data reveal worldwide activity inequality. Nature 2017;547:336-339.
- Kokkinos PF, Faselis C, Myers J, et al. Cardiorespiratory fitness and incidence of major adverse cardiovascular events in US veterans: A cohort study. Mayo Clin Proc 2017;92:39-48.
- Shah RV, Murthy VL, Colangelo LA, et al. Association of fitness in young adulthood with survival and cardiovascular risk: The Coronary Artery Risk Development in Young Adults (CARDIA) study. JAMA Intern Med 2016;176:87-95.
- Tikkanen E, Gustafsson S, Ingelsson E. Associations of fitness, physical activity, strength, and genetic risk with cardiovascular disease: Longitudinal analyses in the UK Biobank study. Circulation 2018;137:2583-2591.
- Pettee Gabriel K, Jaeger BC, Lewis CE, et al. Analysis of cardiorespiratory fitness in early adulthood and midlife with all-cause mortality and fatal or nonfatal cardiovascular disease. JAMA Netw Open 2023;6:e230842.
- Imboden MT, Harber MP, Whaley MH, et al. Cardiorespiratory fitness and mortality in healthy men and women. J Am Coll Cardiol 2018;72:2283-2292.
- Prestgaard E, Hodnesdal C, Engeseth K, et al. Long-term predictors of stroke in healthy middle-aged men. Int J Stroke 2018;13:292-300.
- Wickramasinghe CD, Ayers CR, Das S, et al. Prediction of 30-year risk for cardiovascular mortality by fitness and risk factor levels: The Cooper Center Longitudinal Study. Circ Cardiovasc Qual Outcomes 2014;7:597-602.
- Aitken WW, Brown SC, Comellas AP. Climate change and cardiovascular health. J Am Heart Assoc 2022;11:e027847.
- Vishram-Nielsen JKK, Mueller B, Ross HJ, et al. Association between the incidence of hospitalizations for acute cardiovascular events, weather, and air pollution. JACC Adv 2023;2:100334.
- Basith S, Manavalan B, Shin TH, et al. The impact of fine particulate matter 2.5 on the cardiovascular system: A review of the invisible killer. Nanomaterials (Basel) 2022;12:2656.
- Brook RD, Rajagopalan S, Pope CA 3rd, et al. Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American Heart Association. Circulation 2010;121:2331-2378.
- Alexeeff SE, Liao NS, Liu X, et al. Long-term PM2.5 exposure and risks of ischemic heart disease and stroke events: Review and meta-analysis. J Am Heart Assoc 2021;10:e016890.
- Rajagopalan S, Brauer M, Bhatnagar A, et al. Personal-level protective actions against particulate matter air pollution exposure: A scientific statement from the American Heart Association. Circulation 2020;142:e411-e431.
- Lim CC, Hayes RB, Ahn J, et al. Mediterranean diet and the association between air pollution and cardiovascular disease mortality risk. Circulation 2019;139:1766-1775.
- Krittanawong C, Qadeer YK, Hayes RB, et al. PM2.5 and cardiovascular health risks. Curr Probl Cardiol 2023;48:101670.
- Liu Y, Wheaton AG, Chapman DP, et al. Prevalence of healthy sleep duration among adults — United States, 2014. MMWR Morb Mortal Wkly Rep 2016;65:137-141.
- Watson NF, Badr MS, Belenky G, et al. Recommended amount of sleep for a healthy adult: A joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society. Sleep 2015;38:843-844.
- Wang S, Li Z, Wang X, et al. Associations between sleep duration and cardiovascular diseases: A meta-review and meta-analysis of observational and Mendelian randomization studies. Front Cardiovasc Med 2022;9:930000.
- Fernandez-Mendoza J, He F, Vgontzas AN, et al. Interplay of objective sleep duration and cardiovascular and cerebrovascular diseases on cause-specific mortality. J Am Heart Assoc 2019;8:e013043.
Cardiovascular disease (CVD) is the leading cause of death globally and in the United States. Identifying and targeting cardiovascular risk factors is essential for the prevention and long-term management of CVD. Traditionally, factors for the onset and progression of CVD were thought to be mostly genetic. It is now well established that several of these factors are lifestyle mediated. Behavioral changes significantly influence the interplay between a healthy lifestyle and the genetic risk of heart disease. To further understand the challenges with preventing and reversing CVD, providers need to consider the alarming prevalence of risk factors among the U.S. population.
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.