
By Ashima Goyal Gurkha, DO, FAAP, and Pradeep Padmanabhan, MD, MSc
EXECUTIVE SUMMARY
- Pain is defined as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage. Assessing a child’s pain can be difficult and requires consideration of their age, developmental stage, prior pain experiences, and source of pain.
- Observation-behavior scales have been developed for younger children (< 7 years of age). The widely used Face, Legs, Activity, Cry, Consolability (FLACC) scale is particularly useful in the young.
- Anxiolysis, also termed minimal sedation, is intended to reduce the discomfort of the child mainly through medications, primarily benzodiazepines. Drug-induced anxiolysis or minimal sedation is a state in which the cognition may be impaired without any negative effect on the vital functions (including respiratory and cardiovascular system).
- Lidocaine 2.5% and prilocaine 2.5% (EMLA) is used on closed skin to help with procedural pain, such as prior to a lumbar puncture, intravenous cannulation, or removal of an embedded foreign body (e.g., earrings).
- Nerve blocks work by blocking the transmission of pain impulses through the nerve terminals. Peripheral nerve blocks recently have been used more widely to alleviate pain in fractures, laceration repair, etc. They reduce the need for repeated doses of narcotics and decrease the possibility of serious adverse events, specifically respiratory depression and mental status. The pain control achieved through nerve blocks is significantly better and can last longer.
Any time a child is involved in a traumatic event, they may experience pain or anxiety or both. All providers need to be familiar with the current standard for management of pediatric pain and anxiety, both nonpharmacologic and pharmacologic tools and resources. The authors provide a comprehensive review of an evidence-based approach to the treatment for pediatric pain and anxiety in a child who has experienced trauma.
— Ann M. Dietrich, MD, Editor
Introduction
The fast-paced environment of the emergency department, unfamiliar faces, and noisy surroundings can create challenges when taking care of a child in pain, especially a child who has experienced a traumatic event. Management of pain in pediatric patients requires special considerations because of the unique physiological and psychological needs of children.
Pediatric pain often is underreported and undertreated in spite of various guidelines emphasizing the need for adequate pain control. Adequate pain control is essential in children to avoid long-term negative effects, including increased resistance to future procedures and vaccine hesitancy.1 Studies have shown in children experiencing pain, less than 28% had pain documented and treated with analgesics.2 In addition, oligoanalgesia or inadequate analgesia was common in children treated for long bone fractures, and topical anesthetics were not given during venipunctures in most instances.3
Pain management strategies in pediatrics often involve a combination of pharmacological and non-pharmacological approaches, tailored to the child’s age, developmental stage, and the nature of their pain. Children experience pain differently from adults and, thus, the approach and management must be different. Effective pain management in pediatrics involves a multidisciplinary approach, incorporating both medical and supportive care to address the child’s physical and emotional needs. Pain management in children is a dynamic process that involves assessing pain accurately, choosing appropriate interventions, and continuously evaluating the child’s response to treatment.
Evolution and History of Pain Management
The understanding of pain as a physiological event began in the 1600s. Pain is an event in which the stimulus begins at the surface of the body and travels through the spinal cord to reach a particular site in the brain to generate the perception of discomfort, described as pain.
The emphasis on pain being part of life itself and tolerating pain without medicines was a virtue that has given way to better understanding of the suffering that results from pain. Opioid prescriptions increased initially secondary to cancer-related pain, followed by a more widespread use of opioids for a variety of conditions, followed by an epidemic of addiction. Deaths from overdose, including prescriptions, increased in the 1990s. This was followed by heroin-related deaths. Since 2013, addiction-related deaths have increased dramatically from the use of synthetic opioids, primarily fentanyl, with almost 74,000 overdose deaths in 2022.4
Importantly, there have been misconceptions regarding pain in children. Children often are perceived by some not to remember the painful experiences and as able to tolerate pain more than adults, which is not true.5 It often is difficult to separate anxiety from true pain, and it is important to obtain the parents’ input in such situations. There also is a great reluctance to give narcotics to children, in part from fear of serious side effects. In children, the holistic pain assessment and its management should include crying, inability to sleep, vital sign abnormalities (rapid heart rate, high blood pressure, etc.), and functional limitations in addition to objective assessments, such as pain scores.
Evaluating Pain/Pain Scores
Pain is defined as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage.”6 Acute pain likely is temporary and often results from injury. Chronic pain is persistent and present beyond the expected or usual healing time, such as in juvenile arthritis. It can affect the child’s quality of life and requires ongoing management. Assessing a child’s pain can be difficult and requires consideration of their age, developmental stage, prior pain experiences, and source of pain.
While pain is subjective, it is vital to assess pain as objectively as possible. Pain scores provide vital and primary initial steps to properly alleviate pain. Documentation of pain scores strongly correlates with a child receiving timely and adequate analgesia.7 Pain is unique to each child. Children experience and express pain differently from adults because of their developmental stages, communication abilities, and understanding of pain.
A brief narrative of pain expression through the ages follows.
Neonates and Infants: Pain is expressed through crying, changes in behavior, or physical signs like grimacing/frowning or being angry. They might not be able to verbalize their pain or its intensity (assessment scales include CRIES [Crying, Requiring increased oxygen administration, Increasing {abnormal} vital signs, Expression, Sleeplessness] and Neonatal Infant Pain Scale [NIPS] for children younger than 1 year of age).
Toddlers and Preschoolers: Young children may have a limited understanding of pain and might describe it in simple terms. They often use play or behaviors to express discomfort. Behavioral changes and parents’ perceptions of the presence and severity of pain are important. (An assessment scale example for children older than 1 year of age is FLACC [Face, Legs, Activity, Cry, Consolability] scale.)
School-Age Children: As they get older, children start to have a better understanding of pain and can provide more detailed descriptions. They may use words and often can rate pain using scales (for example, Wong-Baker FACES scale).
Adolescents: An advanced or fully developed ability to understand and articulate pain is noted in adolescents. They can comprehend numeric scales (for example, Numerical Rating Scale [NRS] and Visual Analogue Scale [VAS]) and can discuss the effect of pain on their daily life.
When evaluating pain, age-appropriate pain assessment tools should be considered.8 Observation-behavior scales have been developed for younger children (< 7 years of age). The widely used Face, Legs, Activity, Cry, Consolability (FLACC) scale is particularly useful in the young.9 (See Table 1.) The FLACC scale is a validated, behavioral pain assessment tool designed for use in patients who cannot communicate their pain levels verbally, such as infants, young children (up to 7 years of age), or individuals with cognitive impairments. It provides a systematic way to evaluate pain based on observable behaviors.
Table 1. FLACC (Face, Legs, Activity, Cry, Consolability) Scale | |||
0 | 1 | 2 | |
Face | No expression or smile | Occasional grimace or frown, withdrawn | Frequent or constant frown, clenched jaw |
Legs | Normal position, relaxed | Uneasy, restless, tense | Kicking legs, drawn up |
Activity | Lying quietly, normal position, moves easily | Squirming, shifting back and forth, tense | Arched, rigid, or jerking |
Cry | None | Moaning or whimpering | Crying steadily, screams, sobs, frequent complaints |
Consolability | Content, relaxed | Reassured by occasional touching, hugging, or talking | Difficult to console or comfort |
Scoring: Add the scores from each category. Total score ranges from 0 to 10. 0-3: Mild pain or discomfort 4-6: Moderate pain 7-10: Severe pain Used with permission from: Merkel SI, Voepel-Lewis T, Shaevitz JR, Malviya S. The FLACC: A behavioral scale for scoring postoperative pain in young children. Pediatr Nurs 1997;23:293-297. | |||
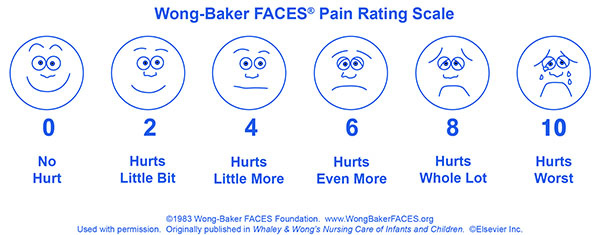
In children older than 8 years of age, self-reporting scales like the Wong-Baker FACES scale or the Numerical Rating Scale often are used.10 (See Figure 1.)
Figure 1. Wong-Baker FACES Pain Rating Scale |
 |
Used with permission. © 1983 Wong-Baker FACES Foundation. |
The child who can understand numbers may rate their pain on a scale from 0 to 10. The Wong-Baker FACES Pain Rating Scale is a visual tool used to help individuals, especially children, communicate their pain levels. It uses a series of six or more faces depicting varying expressions of discomfort, ranging from a happy face (no pain) to a very distressed face (worst pain). The patient is asked to choose the face that best represents how they are feeling. This choice helps healthcare providers assess the level of pain and make decisions about treatment or care. The scale is particularly useful in those who might have difficulty expressing their pain verbally, such as young children or individuals with communication challenges.
In addition to standard pain assessment tools, physiological measures such as monitoring vital signs including heart rate and blood pressure, can help. Changes in these parameters (high heart rate, etc.) sometimes can indicate pain, although they are not specific to pain alone and can be influenced by other factors.
Key considerations for selection of pain assessment tool include the patient’s developmental stage and choosing a tool appropriate for their age and developmental level. Often, a combination of tools and observations provides the most accurate assessment of a child’s pain. Reassessment of a patient’s pain throughout the patient’s encounter is important to ensure appropriate management. Parents and caregivers can provide valuable insights into the child’s pain behavior and symptoms, especially when the child is too young to communicate effectively. Hence, their presence, especially during painful encounters, is warranted. Accurate pain assessment is crucial for effective pain management and improving the overall care and comfort of pediatric patients.
Cultural perceptions also play a role in a child’s perception of pain, expression, and response to pain. Different cultures have varying beliefs about the nature of pain, which can shape how children understand and interpret their pain. For example, some cultures may view pain as a normal part of life, while others may see it as a sign of weakness or failure.11 Some may believe that suffering has a spiritual purpose or that it is a test of faith, affecting how children respond to pain. Different cultures have distinct norms regarding emotional expression. In some cultures, expressing pain openly is encouraged, while in others, children may be trained from a young age to not show vulnerability. This can lead to underreporting of pain. Understanding a child’s cultural background is essential for pain assessment and effective treatment.
Influence of Age/Maturity and Non-Pharmacological Pain Management
Pain management in children is not limited to administration of medications. Studies have shown the benefits of using non-pharmacological methods and interventions, which include reduction in pain, distress, and anxiety as reported by the parent, child, and/or observer.12 These interventions often are neglected as staff members are limited by time restraint and/or are unfamiliar with techniques. Techniques vary based on a child’s age and can be used to help alleviate pain prior to a procedure. General techniques include distraction (toys, videos), comforting touch (massages), tactile comfort (heat/cold therapy, Buzzy), controlled breathing (bubbles, breathing exercises), relaxation (music), and psychology (cognitive behavioral therapy, guided imagery). These techniques can be further implemented by the guidance of a child life specialist.
Infants
Even though infants cannot verbalize pain, they perceive pain and can have memories of pain with lasting effects.13 Some environmental techniques to help infants can include swaddling, music therapy, facilitated tucking, and/or skin-to-skin holding. Swaddling involves wrapping infants in blankets, which can help simulate the environment of the womb and translate to analgesia.14 Encouraging the parent to comfort an infant before and after a painful procedure can help. Music can help grab an infant’s attention and distract from pain. Facilitated tucking involves holding infants in a flexed position with the limbs close to the trunk. This can have an analgesic effect, helping decrease pain signals to the central nervous system.14 Skin-to-skin holding by the child’s mother can have a calming effect. Feeding methods include breastfeeding or non-nutritive sucking with use of a pacifier, which can have a pain-relieving effect.
Oral sucrose solution has been shown to help with temporarily decreasing short-term pain for minor procedures, such as lumbar puncture or venipuncture.15 It has been reported that the optimal pain control is achieved by either administering sucrose on the tongue followed by pacifier or by giving a pacifier dipped in sucrose solution.16,17 Sucrose’s effect can be further enhanced by swaddling. The sweetness of sucrose is thought to activate specific taste receptors that can stimulate release of endorphins and other natural analgesics.15
Toddlers
In this age group, children prefer independence as they enjoy exploring the world around them, and, hence, strategies include distraction, art/music, cold/heat, and/or pet therapy. Distraction with colorful objects, noises, or bubbles can be helpful to grab the toddler’s attention away from his or her pain. Mechanical vibrating devices (e.g., Buzzy) have a vibrating sensation with a friendly animal face that can distract from the sensation of pain when performing procedures such as venipuncture. Art and music therapy can help promote a positive mood and help cope with stress. Cold/heat therapy includes use of an ice pack or heating pack to help with distraction of pain for short periods of time. Pet therapy with the use of dogs can help create a sense of calmness in a young child.
School-Age
School-age children have a better understanding of pain and are active learners. If children can anticipate the next steps, they are better prepared and have lower levels of stress and pain. Some techniques to assist with this include explaining the procedure step by step and using pictures or drawings when available. It also is helpful to allow the child to ask questions and meet with the person who will be performing the procedure. At times, letting a child play the procedure on a doll or watch a demonstration on a doll can help. For example, prior to obtaining an intravenous line (IV), a child can be given a syringe with water to allow them to play and see what the IV will be used for. Children also can be guided through breathing exercises prior to a painful procedure, which can help them calm down.
Adolescents
Adolescents value their independence and prefer to choose the method tool(s), which allows them to cope with pain. Techniques such as distraction can be used with electronic devices, music via headphones, or journaling. Guided imagery and/or cognitive behavioral therapy can be considered but this requires more training and may not be appropriate for an acute setting. Adolescents often seek privacy and therefore, it is important to gain the trust of an adolescent child when treating their pain. Often, talking to an adolescent privately with the parent outside of the room can help identify non-pharmacological interventions that can help them cope with pain.
Anxiolysis
In recent decades, emphasis has been placed not only on the quality of care and the adequate completion of the procedure but also on the physiological outcome, including parental and patient comfort. Young animals exposed to pain and anesthetic procedures have long-term behavioral changes, including memory loss, and are less able to perform tasks compared to peers.18 Similar issues have been noted in children who have undergone multiple surgical procedures.
The presence of parents during procedures, especially at the onset, does seem to diminish anxiety in children. However, studies have noted that pharmacologic agents lessen anxiety far greater than other techniques and, hence, play a greater role.19
Anxiolysis, also termed minimal sedation, is intended to reduce the discomfort of the child mainly through medications, primarily benzodiazepines. Drug-induced anxiolysis or minimal sedation is a state in which the cognition may be impaired without any negative effect on the vital functions (including respiratory and cardiovascular system). It is not intended for children to go to sleep or lose consciousness. Most children are awake during anxiolysis.
The anxiolytic measures often are supplemented by pain medications, including narcotics for painful procedures, but anxiolytic measures help in the initial steps of the procedure. Relatively painless procedures (e.g., nasal foreign body removal) greatly benefit from anxiolysis in children. In addition to benzodiazepines (typically given intranasally or orally), distraction techniques also can reduce anxiety. Anxiety and pain often overlap. Children receiving nasal midazolam with an atomizer (0.3 mg/kg; max dose 10 mg) achieve anxiolysis after five minutes, and the effect is present for about 23 minutes, adequate for short procedures. In the emergency department (ED) setting, it is preferable not to repeat medications intended for anxiolysis unless 30 minutes has elapsed. Intranasal Versed, when properly used with appropriate analgesics, either topical (LMX; lidocaine, epinephrine, tetracaine [LET]), local (lidocaine), or oral medicines (acetaminophen, ibuprofen, and narcotics), can be very effective in comfort for the child and ease of the procedure. Distraction techniques, employed by child life services using videos and toys have been tried. They have not been proven to be effective enough to replace pharmacologic measures, but they can help in simple minimally painful procedures (e.g., IV placement).
Following is the link to an anxiolysis algorithm: https://www.mdanderson.org/documents/for-physicians/algorithms/clinical-management/clin-management-anxiolysis-web-algorithm.pdf
Pharmacological Management
Pain medications are essential and are categorized into different classes based on mechanism of action, including non-opioid analgesics, opioid analgesics, muscle relaxants, and corticosteroids. See Table 2 for drug doses, route of administration, and important considerations. Table 3 lists pharmacological interventions based on pain severity.
Table 2. Pain Medications: Indications and Considerations | |||
Drug | Dose | Common Indications | Important Considerations |
Ibuprofen | PO: 10 mg/kg every 6 h (max dose 800 mg) IV: 10 mg/kg every 6 h (max dose 400 mg) (Not to exceed 40 mg/kg/day or 2,400 mg/day) | Pain relief and antipyretic | Avoid in children younger than 6 months of age because it can cause renal toxicity |
Acetamino-phen | PO: 15 mg/kg every 4 h (max dose 1,000 mg) IV: 15 mg/kg every 6 h (max dose 1,000 mg) (Not to exceed 75 mg/kg/day or 3,750 mg/day) | Pain relief and antipyretic | Is well tolerated by children, can consider use of suppository |
Morphine | IV: 0.05 mg/kg to 0.1 mg/kg q 2-4 hr PO: 0.3 mg/kg q 3-4 hr | Severe pain | Caution with weight-based dosing. Cautious administration to avoid respiratory depression |
Fentanyl | IV: 0.5 mcg/kg to 1 mcg/kg q 30-60 minutes | Severe pain | Can be given intranasally for pain |
Ketamine | IV: 0.05-15 mg/kg/h (max dose 0.5 mg/kg/h) IN: 1 mg/kg (max dose 100 mg) | Pain, sedation | Causes dissociative amnesia, not recommended in children < 3 months of age |
Midazolam | PO: 0.5 mg/kg to 0.7 mg/kg (max 15 mg) IN: 0.3 mg/kg to 0.5 mg/kg (max 10 mg) | Anxiolytic | Can be given intranasally or orally to help calm a patient |
Ketorolac | IV: 0.5 mg/kg every 6 h (max dose 15 mg) Not to exceed 5 days | Moderate/severe pain, migraines | Use with caution in children because it can inhibit platelet function and can cause nephrotoxicity and gastrointestinal disturbance |
PO: per os; IV: intravenous; IN: intranasal; q: every Sources: Chumpitazi CE, Chang C, Atanelov Z, et al. Managing acute pain in children presenting to the emergency department without opioids. J Am Coll Emerg Physicians Open 2022;3:e12664; Stanford Pediatric Pain Service. Pediatric pain pocket reference. https://med.stanford.edu/content/dam/sm/pedsanesthesia/documents/pediatric-pain-pocket-reference.pdf Cote CJ, Wilson S. Guidelines for monitoring and management of pediatric patients during and after sedation for diagnostic and therapeutic procedures: An update. Pediatrics 2006;18:2587-2602. | |||
Table 3. Pharmacological Interventions (Based on Pain Severity) |
Mild Pain
Moderate Pain
Severe Pain
|
Ibuprofen
Mechanism: Ibuprofen, 2-(4-isobutylphenyl) propionic acid, belongs to the class of drugs called nonsteroidal anti-inflammatory drugs (NSAIDs). It works by inhibiting the cyclooxygenase (COX) enzymes, specifically COX-1 and COX-2. These enzymes are involved in the production of prostaglandins, which are compounds that mediate pain, inflammation, and fever.
Routes and Indications: It is commonly available in tablets, capsules, liquid suspensions, and topical gel. It helps with fever reduction, inflammation, and pain relief.
Caution/Interactions: Combining ibuprofen with alcohol can increase the risk of gastrointestinal bleeding.
Contraindications: There have been some reports that NSAID use in the second half of pregnancy may affect the fetal kidneys and the amount of amniotic fluid.20,21
Toxicity: Symptoms of ibuprofen toxicity are unlikely at doses of less than 100 mg/kg in children, and more than 400 mg/kg is associated with serious or life-threatening toxicity. No specific cutoff distinguishes asymptomatic from symptomatic overdose in adults, making the diagnosis challenging. Mild to moderate toxicity includes gastrointestinal symptoms (nausea, vomiting, diarrhea, abdominal pain) and central nervous system effects (headache, dizziness, tinnitus). Severe toxicity can result in acute kidney injury, gastrointestinal bleeding, and confusion.
Ibuprofen should not be given to children younger than 6 months of age because of the risk of serious renal injury. Of note, ibuprofen is not recommended for use after week 20 of pregnancy.
Acetaminophen
Mechanism: N-acetyl-para-aminophenol (paracetamol, APAP) induces analgesia by blocking prostaglandin synthesis from arachidonic acid by inhibiting the enzymes COX-1 and COX-2.
Routes and Indications: It is available in various forms, including tablets, liquid suspensions, IV, and suppositories. In 2010, acetaminophen was approved to be given intravenously in children older than 2 years of age. It can be used for pain relief and fever reduction. Acetaminophen lacks anti-inflammatory effects.
Caution/interactions: Common adverse effects include skin rash, hypersensitivity reaction, and electrolyte imbalances. Acetaminophen should be used cautiously in patients with liver disease or chronic alcohol use because the medication primarily undergoes hepatic metabolism via first-order kinetics. It can interact with other medications, such as blood thinners, increasing bleeding risk. Inducers of CYP2E1, such as isoniazid, phenobarbital, and rifampicin, can increase the metabolism of acetaminophen into toxic N-acetyl-p-benzoquinone imine (NAPQI). Furthermore, many over-the-counter products, including cough and cold medications, include acetaminophen; therefore, cumulative dosing from multiple sources can lead to overdose.
Toxicity: Symptoms of acetaminophen poisoning can vary based on the amount ingested and the timing of the overdose. The Rumack-Matthew Nomogram is the gold standard to predict the likelihood of hepatic failure based on acetaminophen level following a one-time ingestion. An acetaminophen level is obtained four to 24 hours after the time of ingestion and if the level falls above the treatment line, the patient is at risk for liver failure and should be treated with N-acetylcysteine (NAC). A level greater than 150 mcg/mL at four hours from ingestion is considered toxic.23 Indications for NAC include serum levels that fall in the toxic range according to the Rumack-Matthew nomogram, an acetaminophen level greater than 10 mcg/mL with an unknown time of ingestion, a dose of acetaminophen greater than 140 mg/kg taken more than eight hours ago, abnormal laboratory values with ingestion more than 24 hours ago, and ingestion with any evidence of liver injury.
Acetaminophen is particularly useful in children with vomiting because it is available as a suppository. Intravenous acetaminophen can help in severe pain and can be opioid-sparing. Caution should be exercised in interpreting levels in chronic or subacute ingestions because serious toxicity can occur at low serum levels. The nomogram is useful only for acute ingestions.
Aspirin
Mechanism: Acetylsalicylic acid works primarily by inhibiting cyclooxygenase enzymes COX-1 and COX-2. It is an irreversible inhibitor of COX-1 enzyme, unlike ibuprofen, which is a reversible inhibitor. In low doses, aspirin reduces the formation of thromboxane A2, inhibits platelet aggregation, and can reduce the risk of blood clots. By inhibiting COX-2, it reduces pain and inflammation.
Routes and Indications: It is available in various forms, including tablets, chewable tablets, and suppositories. It also is widely available over the counter and found in many formulations, including oil of wintergreen and bismuth subsalicylate.
Caution/Interactions: Aspirin can increase the risk of bleeding when used with anticoagulants like warfarin. The use of aspirin with NSAIDs can increase the risk of gastrointestinal side effects.
Toxicity: Overdose can lead to a mixed acid-base disturbance. Salicylates can lead to direct stimulatory effect on the medullary respiratory center, which causes hyperventilation and tachypnea leading to a respiratory alkalosis. Salicylates also can uncouple oxidative phosphorylation, which leads to a buildup of metabolic products causing metabolic acidosis.24
Aspirin is seldom used in children for analgesia or fever relief. Aspirin may be useful in select situations for its anti-inflammatory properties and cardiovascular protection (clot prevention) in children who have Kawasaki disease.
Opioids
Morphine
Mechanism: Morphine primarily binds to specific receptors in the brain, inhibiting transmission of pain receptors. Morphine, a mu opioid receptor agonist, is the most widely used and studied opioid in children.25 It has been shown to be effective and safe in children of all ages with accepted dosing regimens.
Route and Indications: Various routes exist including oral, IV, and intramuscular (IM). Its indication is for moderate or severe acute pain.
Caution: High-risk groups include neonates and those with obstructive sleep apnea, severe neurodevelopmental conditions, trisomy 21, and severe epilepsy.
Toxicity: Morphine is associated with histamine release, causing mild symptoms such as itching and rash to the more serious hypotension from vasodilation. Young children, particularly infants and neonates, may have heightened sensitivity to opioids because of immature liver and kidney function affecting drug metabolism and clearance. Young children may not develop the same degree of tolerance as adults, making them more susceptible to the effects of opioids at lower doses. Slow-release opioids or opioids that are given quickly at high doses can cause respiratory depression.
Morphine is safe at all ages. However, one should exercise caution in dosing morphine in neonates and young infants because of the risk of respiratory depression.
Fentanyl
Mechanism: The mechanism is similar to other opioids in which it stimulates mu-opioid receptors in the central nervous system. Fentanyl is a very potent opioid, approximately 50-100 times more potent than morphine. Compared to morphine, fentanyl has very little effect on histamine release.26
Route and Indications: Fentanyl can be given through multiple routes, including IV, IM, transdermal, and transmucosal/intranasal routes.
Transdermal Fentanyl: Transdermal patches of fentanyl offer significant pain relief with bioavailability close to 80%. These are selectively used in older children/adolescents with severe chronic pain and in palliative settings. Fentanyl continues to be absorbed from skin even after a patch is removed. Accidental ingestion of a single patch of fentanyl (even if previously used) by young children can be lethal and, hence, caution should be exercised in keeping fentanyl patches out of reach. The patches should be disposed of carefully and flushed in the toilet. Naloxone should always be available to those using transdermal patches in case of overdose/serious side effects.
Transmucosal/Intranasal Fentanyl: Intranasal (IN) fentanyl is a very effective drug for acute severe pain in children, such as fractures. Fentanyl intranasally is as effective as IV morphine, can be given promptly, and obviates the need for IV placement in children already in severe pain and discomfort. This is the preferred drug for acute severe pain in children’s hospitals.27 Fentanyl IN can be given safely to children as young as 12 months of age and during prehospital care.28
Toxicity: Nonprescription fentanyl use is a serious public health emergency. Overdose of fentanyl can result in respiratory depression and central nervous system (CNS) depression. A unique severe complication of fentanyl is a life-threatening chest wall rigidity even at therapeutic doses.
Intranasal fentanyl is safe and is the preferred first-line drug in severe pain associated with burns or fractures. Fentanyl is rarely associated with chest wall rigidity. While transdermal patches provide good pain relief, they should be avoided in young children and limited to older adolescents in chronic severe pain. In suspected opioid overdoses, naloxone administration is lifesaving. Chronic prescription users of opioids always should have access to naloxone.
Ketamine
Mechanism: Ketamine is an N-methyl-D-aspartate (NMDA) receptor antagonist. By inhibiting the excitatory neurotransmitter glutamate’s action, ketamine produces both anesthesia and analgesia. It also interacts with opioid receptors, particularly the mu-opioid receptor, which allows for its mood-altering effects.29 Ketamine is a dissociative anesthetic that can induce feelings of detachment from the environment and oneself. Because of its sympathomimetic effects, ketamine can cause a transient increase in heart rate and blood pressure secondary to release of catecholamines. Unlike opioids, it does not produce respiratory depression, decrease airway tone, or cause hypotension.
Route and Indications: Ketamine can be administered several routes, including IV, IM, IN, and oral. It is the most preferred for painful procedures (e.g., fracture reduction) because it supplements optimal pain control with dissociative anesthesia.
Caution/Interactions: Ketamine should be avoided in pediatric patients younger than 3 months of age because there have been limited studies. Caution should be exercised in children with a history of psychiatric disorders because ketamine may exacerbate them. Side effects include the emergence reaction, which is less common in children, and includes terrifying hallucinations and delirium. Ketamine can cause laryngospasm, myoclonic jerks, and/or tremors.
Toxicity: Ketamine can be used recreationally as a drug of abuse, which can lead to toxicity. No antidote is available, with treatment involving supportive care.
Ketamine, a dissociative anesthetic, offers potent analgesia with minimal side effects. It is widely used in fracture reductions and other painful procedures. Ketamine is safe and can be given in multiple routes, including IM and IN routes.
Ketorolac
Mechanism: Ketorolac works by blocking the production of prostaglandins by inhibiting COX-1 and COX-2 enzymes.
Route and Indications: Routes include IV, oral, and IM. Indications include moderate to severe pain management, kidney stones, migraines, and pain from injuries.
Caution/Toxicity: Ketorolac has gained widespread acceptance as a very effective analgesic for acute severe pain primarily because it is a non-narcotic. Ketorolac is widely used in emergency departments. Studies have shown that ketorolac 10 mg intravenously is an effective and an adequate ceiling dose in adults.30
Toxicity: High doses can lead to hepatotoxicity and/or nephrotoxicity. Ketorolac is liberally used and, in most situations, the maximum dose (30 mg IV) is used. Anaphylactic shock also has been noted. Management includes supportive care with no antidote available.31,32
Ketorolac should be used very sparingly for short-term management in children and should not exceed five days to minimize risks of adverse effects. Side effects include but are not limited to gastrointestinal disturbance, renal impairment, and bleeding from platelet dysfunction. Use with extreme caution in children who are receiving aspirin or other NSAIDs.
Ketorolac, a commonly used analgesic in children and is very helpful in addressing severe pain. The drug has potential for significant toxicity and severe side effects. High doses can cause toxicity, which may not be recognized in the acute setting of the emergency department. The dosing should be carefully considered because a lower dose often is equally effective.
Corticosteroids
Mechanism: Corticosteroids are potent anti-inflammatory medications that can be used to manage certain types of pain in pediatric patients. The physiological and pharmacological effects of corticosteroids are mediated by binding to the glucocorticoid receptor.33
Route and Indications: Corticosteroids can be administered orally, intramuscularly, intravenously, or topically, depending on the condition being treated. It is commonly used as an anti-inflammatory drug in asthma and croup. It can be used for severe pain in patients with pharyngitis.
Caution: Children are susceptible to effects on growth and development. Children also may show more pronounced mood or behavior changes, such as irritability and/or agitation. Sudden discontinuation of corticosteroids, especially after long-term use, can precipitate a life-threatening adrenal crisis because of insufficient adrenal hormone levels.
Toxicity: Corticosteroids can cause significant toxicity, particularly with long-term use. Some side effects include rounded face (“moon facies”), weight gain, muscle wasting, acne, bruising, exacerbation of gastroesophageal disease, and development of peptic ulcer.33
Prolonged use of steroids in children is strongly discouraged other than in extenuating circumstances because of the effect on growth and serious side effects.
Topical Analgesia
Topical analgesics are an important noninvasive tool to help alleviate pain and anxiety in children. Transient loss of sensory, motor, and autonomic function occurs when the drug is injected or applied in proximity to neural tissue. Topical anesthetics can play a significant role with local pain control for procedures such as intravenous (IV) access, lumbar puncture, laceration repair, and incision and drainage of abscess and/or wound management. Some examples of topical anesthetics and their role are discussed in the following sections. (See Table 4.)
Table 4. Topical Analgesics Used in the Emergency Department |
Lidocaine (LMX)
Lidocaine and Prilocaine (EMLA)
Lidocaine, Epinephrine, Tetracaine (LET)
Ethyl Chloride Spray
Pentafluoropropane and tetrafluoroethane (Pain Ease)
|
Adapted from: Webb TL, Sanders JE. Pediatric pain. In: Cisewski DH, Motov SM, eds. Pain Management Guide. Emergency Medicine Residents Association; 2020. |
Vapocoolant spray consists of topical ethyl chloride and helps provide transient skin anesthesia within seconds of application. It often is used prior to starting an IV. Prior studies have demonstrated vapocoolant spray quickly and effectively reduced pain from IV cannulation in children and improved the success rate of IV cannulation.34
Lidocaine 4%-epinephrine 0.1%-tetracaine 0.5% gel (LET) is used for lacerations. Time to onset is approximately 30 minutes. The goal of LET is to pretreat the wound to allow for painless administration of an injectable anesthetic. In younger children, LET is commonly used exclusively by itself to pretreat the patient prior to placement of sutures for a laceration repair.
Lidocaine 2.5% and prilocaine 2.5% (EMLA) is used on closed skin to help with procedural pain, such as prior to a lumbar puncture, IV cannulation, or removal of an embedded foreign body (e.g., earrings). The cream is absorbed by the skin and helps anesthetize the nerve endings. Time to onset is approximately 60 minutes.
LMX-4 (45 lidocaine) is a topical lidocaine anesthetic that can help with procedures such as abscess incision and drainage. The analgesia is noted in approximately 30 minutes.
J tip: The J tip is a type of apparatus that uses air instead of a needle to push lidocaine into the skin. It has a curved, blunt tip that resembles the letter “J.” The design allows for a less painful injection compared to traditional sharp needles, making it particularly useful in pediatric patients. It helps to minimize trauma to tissues and blood vessels during injection.35
Nerve Blocks
Nerve blocks work by blocking the transmission of pain impulses through the nerve terminals. Peripheral nerve blocks recently have been used more widely to alleviate pain in fractures, laceration repair, etc. They reduce the need for repeated doses of narcotics and decrease the possibility of serious adverse events, specifically respiratory depression and mental status. The pain control achieved through nerve blocks is significantly better and can last longer. Commonly, lidocaine and mepivacaine are used for short duration procedures. Analgesia can be considerably longer in duration depending on the drug used (e.g., bupivacaine). The effective analgesia achieved with a nerve block can be as long as 16 hours with some measure of pain control even up to three days.
However, nerve blocks should not be performed in infants younger than 6 months of age because they have four times the risk of complications compared to older children and adults.
In the emergency setting, a single dose of the nerve block is most effective. In all patients receiving nerve blocks, an IV line should be placed. Accidental drug delivery intravenously could be catastrophic. Lipid emulsion should always be available for the most serious side effects from nerve blocks described as LAST (local anesthetic systemic toxicity). Severe reactions include seizures, arrhythmias, and cardiac arrest. Serious side effects are treated with benzodiazepines (seizures), antiarrhythmics, and lipid emulsion (cardiac arrest, hypotension, etc.).36 The use of focused ultrasound to guide nerve blocks has significantly reduced the incidence of serious adverse events. Some nerve blocks are discussed in the following sections.
Femoral Nerve Block
The femoral nerve block anesthetizes the femoral nerve distribution and is used for anterior thigh and knee injuries. This is particularly helpful in femur fractures. This should be done meticulously with ultrasound guidance to avoid infiltration into the femoral vessels. As mentioned previously, IV lipids should be readily available in case of this potentially catastrophic side effect. The idea is to infiltrate the femoral sheath lateral to the femoral artery carefully, typically with a large amount of a long-acting anesthetic (e.g., ropivacaine) to ensure adequate and prolonged anesthesia. Properly done femoral block-driven analgesia can last close to 24 hours and may be adequate for corrective orthopedic procedures with minimal additional analgesia.
Facial Blocks
Infraorbital Block
This block is an effective tool for laceration repairs involving the midface below the eyelids (lower half of the face up to the upper lips). The technique involves identifying the infraorbital foramen and injecting typically 1 mL to 2 mL of a short-acting anesthetic through the oral mucosa or externally. For the external technique, the infraorbital foramen can be located along the imaginary straight line going down from the midline pupil to the inferior border of the infraorbital ridge. After cleaning the surface, the anesthetic then is injected in and around the area. For the internal technique, provide topical anesthetic to the mucosa superior to the maxillary canine.
Mental Block
The mental nerve is a branch of the mandibular division of the trigeminal nerve. A mental block provides numbness over the lower lip and chin. The mental foramen is located at the junction of the first and second mandibular premolars, about 1 cm below the gum line. It is in line with the infraorbital foramen. Inject 1 mL to 3 mL of local anesthetic in line with the middle of the body of the mandible. The intraoral approach involves providing topical anesthetic to the mucosa at the junction of the lower canine and first premolar.
Supraorbital Block
A supraorbital block provides numbness over the eyelid, forehead, and scalp. Palpate the supraorbital rim, identify the supraorbital notch, and inject 1 mL to 3 mL of local anesthetic just below the notch to provide pain relief to the areas innervated by the supraorbital nerve, a branch of the trigeminal nerve.
Acupuncture
Acupuncture is an ancient Chinese technique that uses acus (needle) and puncture (precisely placed needles) at specific anatomic points for the desired analgesia. Neurotransmitters such as opioids, serotonin, norepinephrine, orexin, and endocannabinoid are modulated by acupuncture to induce analgesia. Acupuncture has been effective in pain control and is increasingly being used in the ED.37 In addition to analgesia, acupuncture technique has anti-inflammatory properties.
Special Populations
Autism/Developmental Delay
Managing pain in children with autism can be particularly challenging because of difficulties with communication and varying sensory sensitivities. Patients with developmental delay can exhibit pain in a more heightened manner. Children in this population often are not able to verbally communicate their pain. For example, patients with cerebral palsy can present with a smile, laughter, or fussiness, which may be misconstrued and not recognized as a manifestation of pain.38 When assessing pain in patients who are nonverbal or have developmental delay, observational tools can be helpful to assess pain, especially if the individual has limited verbal communication. Changes in behavior, such as increased agitation, withdrawal, or changes in typical routines, can be a helpful clue as a sign of pain. There are modified pain scales or tools adapted for individuals with autism. For example, the Non-Communicating Children’s Pain Checklist or the Pain Assessment in Non-Communicative Children (PANCC) can be useful.39
It is very important to include caregivers in decision-making because they have a better understanding of the patient’s behaviors and painful situations. Opioids can be used for severe pain, if necessary, but should be used cautiously and under supervision. It also is important to remember patients with developmental delay or with a complex medical history may be taking multiple medications. Non-pharmacological strategies that may be effective include sensory integration or comforting activities. The individual’s sensory sensitivities should be considered, and use of weighted blankets or calming sounds can help.
Effective pain management for individuals with autism requires a personalized approach that considers their unique sensory sensitivities, communication challenges, and behavioral responses. Overstimulation should be avoided.
Neonates
Historically, there have been perceptions that neonates are incapable of experiencing pain. These views were based on theories stating neonates had an underdeveloped central nervous system and a lack of pain receptors. However, recent studies highlight that acute pain is activated in the sensory cortex even in premature neonates.40 Neonates can and will experience pain and demonstrate specific pain behaviors. Early periods of development are particularly vulnerable to effects of acute pain exposure.41,42 Pain management in this population requires careful consideration because of their developmental stage and the potential impact of pain and analgesic interventions. Neonates cannot verbally communicate their discomfort; therefore, it is important to look for signs such as facial expression (grimacing), changes in cry pattern (high-pitched, continuous crying), changes in body movement (stiffening, arching), or sleep disturbance. Pain scales designed for neonates include the Neonatal Infant Pain Scale (NIPS), which evaluates facial expression, cry, breathing pattern, arms, legs, and state of arousal, and the Premature Infant Pain Profile (PIPP), which assesses facial expression, heart rate, oxygen saturation, and gestational age.43
Pharmacological pain management includes acetaminophen for mild/moderate pain. For painful procedures such as hernia reduction, morphine can be considered. As mentioned previously, oral sucrose or topical medications such as EMLA may be used for minor procedures to reduce pain at the site. Non-pharmacological considerations include skin-to-skin contact, sucking, and feeding (sucking on a pacifier or during breastfeeding can help soothe pain because of the analgesic effect of sucking and the release of endorphins). Swaddling can provide comfort and a sense of security. Gentle stroking or massage may help alleviate discomfort and provide reassurance.
Chronic Pain
Chronic pain is defined as pain lasting longer than three to six months or beyond the usual time for healing. Age-appropriate pain assessment tools should be considered. Psychosocial assessment should evaluate the emotional, social, and psychological effect of pain as well as family dynamics. It is essential to consider a multimodal approach when approaching a patient with chronic pain.
Patients often had prior unpleasant experiences, which may prime these children to have amplified anxiety and perception of pain.44 Pharmacological management should highlight use of non-opioid analgesics including acetaminophen/ibuprofen in most circumstances, and opioids should be reserved and used sparingly only for severe pain. Topical creams, patches, or gels can be considered for localized pain, when appropriate.
Pediatric palliative care focuses on providing relief from pain and other distressing symptoms for children with serious illnesses. Symptoms that may exacerbate pain, such as nausea, constipation, or dyspnea, should be treated effectively. Individualized care plans should be developed that address the child’s specific symptoms and preferences, including a combination of pharmacological and non-pharmacological approaches. Non-pharmacological measures include physical comfort such as gentle massage, heat/cold therapies, or distraction games and music/art. Regarding respect for autonomy, consider the child’s developmental stage and involve them in decision-making to the fullest extent possible.45
Complex Regional Pain Syndrome (CRPS) is a chronic pain condition that usually affects a limb, such as an arm or leg, and is characterized by severe pain, swelling, and changes in the skin. It is more common among adolescent girls, and lower extremity pain is a typical presentation. The exact mechanism is unknown. Once pediatric CRPS is diagnosed, standard care involves a multidisciplinary approach with intensive physical therapy in conjunction with psychological treatment in addition to analgesics. Treatment should involve consideration of the child and the surrounding environment, family, and academic and social issues. Pharmacological measures may assist in decreasing pain to allow the patient to participate fully in intensive physiotherapy.46
Sickle cell disease and associated severe pain from vaso-occlusive crisis in older children, particularly adolescents, often require emergency department visits. Many children do not have access to prompt medical care, and the severe pain often is ignored or undertreated. These children experience severe pain, and it is important to treat the pain adequately. Patients with sickle cell disease managed by a hematologist often have a pain management plan that is made in conjunction with the patient, caregiver, and their care team. Adherence to this plan can be very effective in alleviating pain.47
Chronic pain management involves a multimodal approach, including addressing pain with preferably a treatment plan and ensuring the patient’s compliance with the home treatment regimen. It is paramount to recognize the severity of acute on chronic pain and care for the patients with kindness while ensuring that long-term harm is not caused.
Summary
Children offer unique challenges in the evaluation and management of pain. Pediatric patients, including neonates, do experience pain. The pain control often is achieved with reduction of anxiety and use of non-pharmacologic measures (e.g., distraction) in addition to medications. The medications should be carefully titrated for the child to prevent serious side effects. In situations involving chronic pain, clinicians should not underestimate or ignore the pain and should be diligent in using a multimodal plan for pain control.
Ashima Goyal Gurkha, DO, FAAP, is a pediatric emergency medicine physician with Dayton Children’s Hospital in Dayton, OH. Pradeep Padmanabhan, MD, MSc, is Associate Pediatric Emergency Medicine Fellowship Director, Dayton Children’s Hospital, Dayton, OH.
References
1. Noel M, Chambers CT, McGrath PJ, et al. The influence of children’s pain memories on subsequent pain experience. Pain. 2012;153(8):1563-1572.
2. Stevens BJ, Abbott LK, Yamada J, et al. Epidemiology and management of painful procedures in children in Canadian hospitals. CMAJ. 2011;183(7):E403-E410.
3. Noble J, Zarling B, Geesey T, et al. Analgesia use in children with acute long bone fractures in the pediatric emergency department. J Emerg Med. 2020;58(3):500-505.
4. National Institute on Drug Abuse. Drug overdose deaths: Facts and figures. https://nida.nih.gov/research-topics/trends-statistics/overdose-death-rates
5. Gallastegui-Brana A, Rodríguez-Nunez A, Palacios J, et al. Development and validation of a tool to assess the structural quality of palliative care services. J Pain Symptom Manage. 2023;65(6):490-499.e50.
6. Rosen DM, Alcock MM, Palmer GM. Opioids for acute pain management in children. Anaesth Intensive Care. 2022;50(1-2):81-94.
7. Kellogg KM, Fairbanks RJ, O’Connor AB, et al. Association of pain score documentation and and analgesic use in a pediatric emergency department. Pediatr Emerg Care. 2012;28:1287-1292.
8. Webb T, Sanders J. Chapter 12- Pediatric Pain. In: Pain Management Guide, 1st ed. Emergency Medicine Residents Association; 2020. https://www.emra.org/books/pain-management/pediatric-pain
9. Merkel SI, Voepel-Lewis T, Shayevitz JR, Malviya S. The FLACC: A behavioral scale for scoring postoperative pain in young children. Pediatric Nursing. 1997;23(3):293-297.
10. Garra G, Singer AJ, Taira BR, et al. Validation of the Wong-Baker FACES Pain Rating Scale in pediatric emergency department patients. Acad Emerg Med. 2010;17(1):50-54.
11. Finley GA, Kristjánsdóttir O, Forgeron PA. Cultural influences on the assessment of children’s pain. Pain Res Manag. 2009;14(1):33-37.
12. Wente SJ. Nonpharmacologic pediatric pain management in emergency departments: A systematic review of the literature. J Emerg Nurs. 2013;39(2):140-150.
13. Porter FL, Grunau RE, Anand KJ. Long-term effects of pain in infants. J Dev Behav Pediatr. 1999;20(4):253-261.
14. Mangat AK, Oei JL, Chen K, et al. A review of non-pharmacological treatments for pain management in newborn infants. Children (Basel). 2018;5(10):130.
15. Harrison D, Beggs S, Stevens B. Sucrose for procedural pain management in infants. Pediatrics. 2012;130(5):918-925.
16. Gibbins S, Stevens B, Hodnett E, et al. Efficacy and safety of sucrose for procedural pain relief in preterm and term neonates. Nurs Res. 2002;51(6):375-382.
17. Stevens B, Johnston C, Franck L, et al. The efficacy of developmentally sensitive interventions and sucrose for relieving procedural pain in very low birth weight neonates. Nurs Res. 1999;48(1):35-43.
18. Disma N, O’Leary JD, Loepke AW, et al. Anesthesia and the developing brain: A way forward for laboratory and clinical research. Paediatr Anaesth. 2018;28(9):758-763.
19. Manyande A, Cyna AM, Yip P, et al. Non-pharmacological interventions for assisting the induction of anaesthesia in children. Cochrane Database Syst Rev. 2015;2015(7):CD006447.
20. Drukker A. The adverse renal effects of prostaglandin-synthesis inhibition in the fetus and the newborn. Paediatr Child Health. 2002;7(8):538-543.
21. Leverrier-Penna S, Michel A, Lecante LL, et al. Exposure of human fetal kidneys to mild analgesics interferes with early nephrogenesis. FASEB J. 2021;35(7):e21718.
22. Chumpitazi CE, Chang C, Atanelov Z, et al. Managing acute pain in children presenting to the emergency department without opioids. J Am Coll Emerg Physicians Open. 2022;3:e12664.
23. Agrawal S, Khazaeni B. Acetaminophen Toxicity. In: StatPearls [Internet]. StatPearls Publishing; 2024 Jan-. Updated June 9, 2023. https://www.ncbi.nlm.nih.gov/books/NBK441917
24. Arif H, Aggarwal S. Salicylic Acid (Aspirin). In: StatPearls. StatPearls Publishing; Updated July 5, 2023.
25. Verghese ST, Hannallah RS. Acute pain management in children. J Pain Res. 2010;3:105-123.
26. Rosow CE, Moss J, Philbin DM, Savarese JJ. Histamine release during morphine and fentanyl anesthesia. Anesthesiology. 1982;56(2):93-96.
27. Borland M, Jacobs I, King B, O’Brien D. A randomized controlled trial comparing intranasal fentanyl to intravenous morphine for managing acute pain in children in the emergency department. Ann Emerg Med. 2007;49(3):335-340.
28. Cole J, Shepherd M, Young P. Intranasal fentanyl in 1-3-year-olds: A prospective study of the effectiveness of intranasal fentanyl as acute analgesia. Emerg Med Australas. 2009;21:395-400.
29. Gregers MCT, Mikkelsen S, Lindvig KP, Brøchner AC. Ketamine as an anesthetic for patients with acute brain injury: A systematic review. Neurocrit Care. 2020;33(1):273-282.
30. Motov S, Yasavolian M, Likourezos A, et al. Comparison of intravenous ketorolac at three single-dose regimens for treating acute pain in the emergency department: A randomized controlled trial. Ann Emerg Med. 2017;70(2):177-184.
31. Soleyman-Zomalan E, Motov S, Likourezos A, et al. Patterns of ketorolac dosing by emergency physicians. World J Emerg Med. 2017;8(1):43-46.
32. Mahmoodi AN, Patel P, Kim PY. Ketorolac. In: StatPearls. StatPearls Publishing. Updated Feb. 28, 2024.
33. Ferrara G, Petrillo MG, Giani T, et al. Clinical use and molecular action of corticosteroids in the pediatric age. Int J Mol Sci. 2019;20(2):444.
34. Farion KJ, Splinter KL, Newhook K, et al. The effect of vapocoolant spray on pain due to intravenous cannulation in children: A randomized controlled trial. CMAJ. 2008;179(1):31-36.
35. Lunoe MM, Drendel AL, Levas MN, et al. A randomized clinical trial of jet-injected lidocaine to reduce venipuncture pain for young children. Ann Emerg Med. 2015;66(5):466-474.
36. Torp KD, Metheny E, Simon LV. Lidocaine Toxicity. In: StatPearls [Internet]. StatPearls Publishing; 2024 Jan-. Updated Dec. 8, 2022. https://www.ncbi.nlm.nih.gov/books/NBK482479/
37. Grissa MH, Baccouche H, Boubaker H, et al. Acupuncture vs intravenous morphine in the management of acute pain in the ED. Am J Emerg Med. 2016;34:2112–2116.
38. Hadden KL, von Baeyer CL. Pain in children with cerebral palsy: Common triggers and expressive behaviors. Pain. 2002;99(1-2):281-288.
39. Breau LM, Finley GA, McGrath PJ, Camfield CS. Validation of the non-communicating children’s pain checklist-postoperative version [published correction appears in Anesthesiology. 2002 Sep;97(3):769]. Anesthesiology. 2002;96(3):528-535.
40. Bartocci M, Bergqvist LL, Lagercrantz H, Anand KJ. Pain activates cortical areas in the preterm newborn brain. Pain. 2006;122(1-2):109-117.
41. Perry M, Tan Z, Chen J, et al. Neonatal pain: Perceptions and current practice. Crit Care Nurs Clin North Am. 2018;30(4):549-561.
42. Fitzgerald M. What do we really know about newborn infant pain? Exp Physiol. 2015;100(12):1451-1457.
43. Sarkaria E, Gruszfeld D. Assessing neonatal pain with NIPS and COMFORT-B: Evaluation of NICU’s staff competences. Pain Res Manag. 2022;2022:8545372.
44. Cornelissen L, Donado C, Kim J, et al. Pain hypersensitivity in juvenile idiopathic arthritis: A quantitative sensory testing study. Pediatr Rheumatol Online J. 2014;12:39.
45. Downing J, Jassal SS, Mathews L, et al. Pediatric pain management in palliative care. Pain Manag. 2015;5(1):23-35.
46. Weissmann R, Uziel Y. Pediatric complex regional pain syndrome: A review. Pediatr Rheumatol Online J. 2016;14(1):29.
47. Zempsky WT. Evaluation and treatment of sickle cell pain in the emergency department: Paths to a better future. Clin Pediatr Emerg Med. 2010;11(4):265-273.