How Many Abnormal Findings?
By Ken Grauer, MD
Professor Emeritus in Family Medicine, College of Medicine, University of Florida
No history was available for the tracing in the figure below. There are at least seven ECG findings to note. How many can you identify?
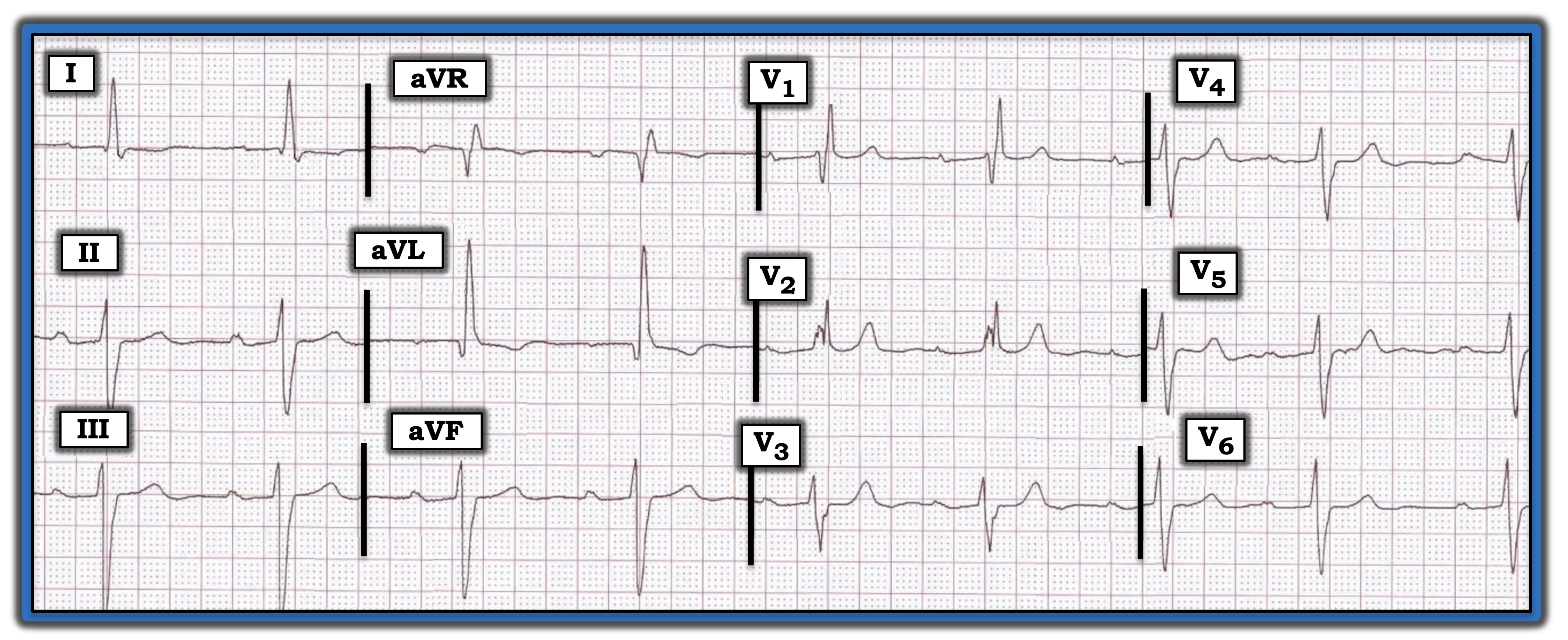
Interpretation: It always is challenging to interpret a tracing without the benefit of any clinical history. That said, there are some findings here that should help. Although there is no long lead rhythm strip, the upright P wave with fixed PR interval in lead II identifies the underlying rhythm as sinus. It appears that each QRS complex is preceded by a P wave with similar PR interval.
Even without the benefit of a long lead rhythm strip, it appears the rate is slow and irregular (i.e., one of the R-R intervals in lead V6 is six large boxes, whereas the other is five large boxes). Therefore, there is sinus bradycardia and arrhythmia (with a heart rate between ~50 beats per minute and 60 beats per minute).
The PR interval clearly is prolonged (i.e., to ~0.32 seconds), indicating there is first-degree AV block. The QRS complex is wide (i.e., between 0.12 seconds and 0.13 seconds in duration). QRS morphology is consistent with right bundle branch block (RBBB) in that there is an rSR’ complex in lead V1 with wide terminal S waves in lateral leads I and V6.
There also is left anterior hemiblock (LAHB), as determined by a frontal plane axis that is more negative than -30° (i.e., predominant negativity in each of the inferior leads). There is left ventricular hypertrophy, as determined by the towering R wave in lead aVL that exceeds 12 mm in amplitude.
The Q wave in lead aVL is abnormally wide. This suggests that rather than a “normal septal q wave,” this Q wave in lead aVL may be a marker of prior infarction.
Finally, there are primary ST-T wave changes in the anterior leads. Normally, with RBBB, ST-T waves are depressed in the anterior leads. Instead, there is abnormal ST segment straightening in leads V3-V6, and distinctly abnormal upright and peaked T waves that begin in lead V1 and persist through to lead V6.
Putting It All Together: Clinical correlation is essential for determining the significance of these findings. The slow heart rate with multiple conduction defects (first-degree AV block, RBBB, LAHB) are of concern and would be especially worrisome if the history indicated syncope and/or recent chest pain.
For more information about and further discussion of this case, please click here.
No history was available for the tracing in the figure. There are at least seven ECG findings to note. How many can you identify?
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.