
By Ken Grauer, MD
You are given the electrocardiogram (ECG) in the figure without the benefit of any history.
- How would you interpret this tracing?
- How does the 12-lead ECG help with interpretation of the rhythm?
Interpretation: I began my interpretation of today’s tracing by looking at the long lead II rhythm strip.
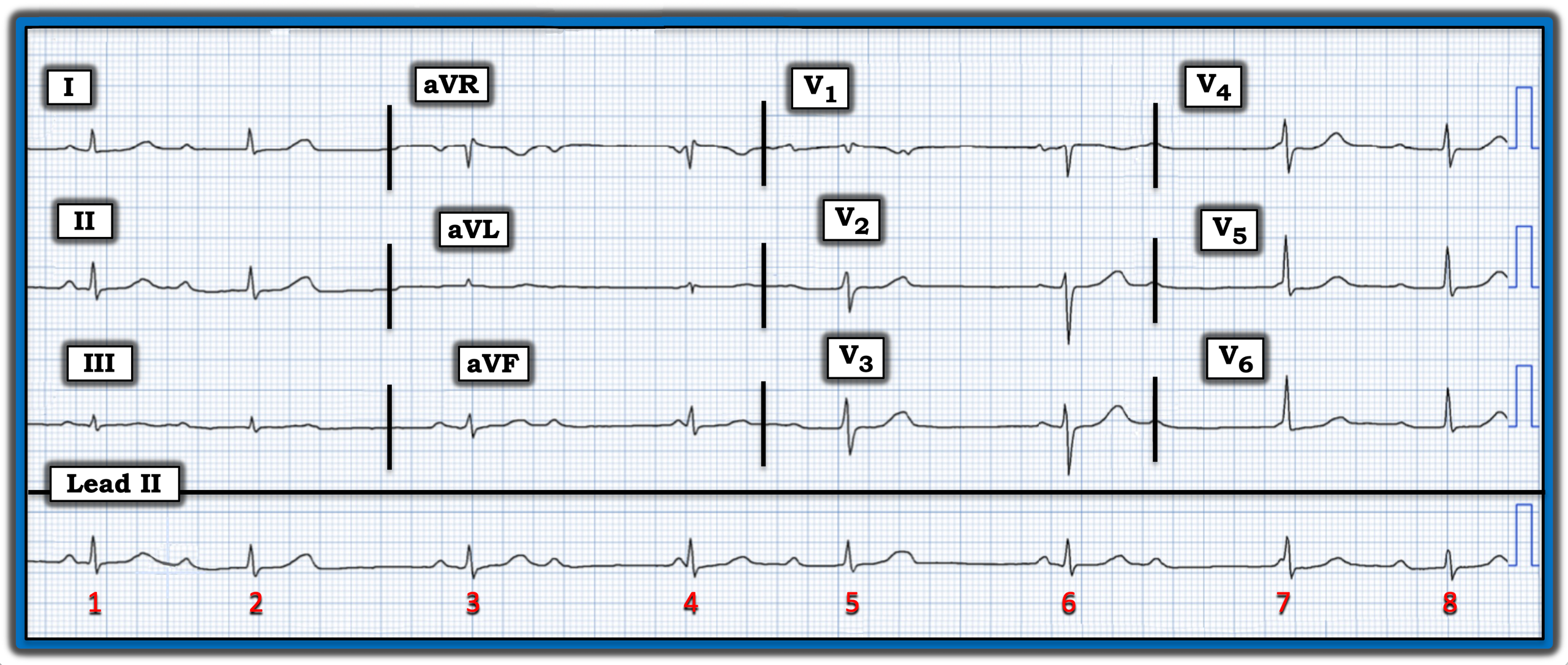
- The QRS is narrow — so the rhythm is supraventricular.
- The rhythm is not regular. Instead, there are two basic groups of beats — with either longer or shorter R-R intervals (i.e, the R-R intervals between beats 1-2, 4-5, and 7-8 are all similar, and the longer R-R intervals between beats 2-3, 3-4, 5-6, and 6-7 are all of similar duration).
- P waves are present. Although difficult to be certain without calipers, I suspect the reason the T waves of beats 2 and 5 are “fatter” is that on-time P waves are hidden within these T waves. If so, then the atrial rhythm is most probably regular enough to qualify as sinus arrhythmia.
- Whenever you see “group beating” in association with an underlying regular (or almost regular) sinus rhythm, consider the possibility of AV Wenckebach (second-degree AV block, Mobitz Type I).
- The PR interval before narrow beats 4 and 7 clearly is too short to consider conduction. Since the QRS complex of these beats is narrow, beats 4 and 7 must be junctional escape beats. And since the R-R interval preceding beats 4 and 7 is similar to the R-R interval before beats 3 and 6, it is likely that beats 3 and 6 are also junctional escape beats.
- In contrast, beats 2, 5 and 8 all occur earlier than expected. This suggests that, even though the PR interval before these beats varies, it is likely that beats 2, 5, and 8 are all probably conducted, albeit with first-degree AV block.
How does the 12-lead ECG help with interpretation of the rhythm?
- Note how flat the ST-segments are in leads V2 and V3. Normally, there should be a slight, upward-sloping ST-elevation in these two leads. If this patient had recent chest pain, acute posterior infarction would need to be considered, since this is a common cause of ST depression (or inappropriate ST flattening) that is maximal in leads V2, V3, and/or V4.
Impression: This is a very challenging ECG — especially since we are not provided with any clinical history. That being said, the finding of “group beating” in a supraventricular rhythm in which there is an underlying sinus rhythm with conducted beats manifesting first-degree AV block immediately should suggest the possibility of second-degree AV block, Mobitz Type I.
- The most common setting for AV Wenckebach is acute or recent inferior and/or posterior infarction. Therefore, the moment I saw the inappropriate ST-segment flattening that was most marked in leads V2 and V3, I immediately suspected AV Wenckebach as a result of recent posterior infarction.
- The reason today’s rhythm is so challenging is that we see multiple junctional escape beats that mask what otherwise would be the typical picture of Mobitz I (i.e., with progressive PR interval prolongation until a beat is dropped).
Note: For more information about this case, visit https://tinyurl.com/KG-Blog-421.
You are given the electrocardiogram (ECG) in the figure without the benefit of any history. How would you interpret this tracing? How does the 12-lead ECG help with interpretation of the rhythm?
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.