Double BBB, or Complete AV Block?
By Ken Grauer, MD
Professor Emeritus in Family Medicine, College of Medicine, University of Florida
The ECG in the figure below is from a woman who complained she had been experiencing chest pain for several days. What is the rhythm? Is there complete AV block?
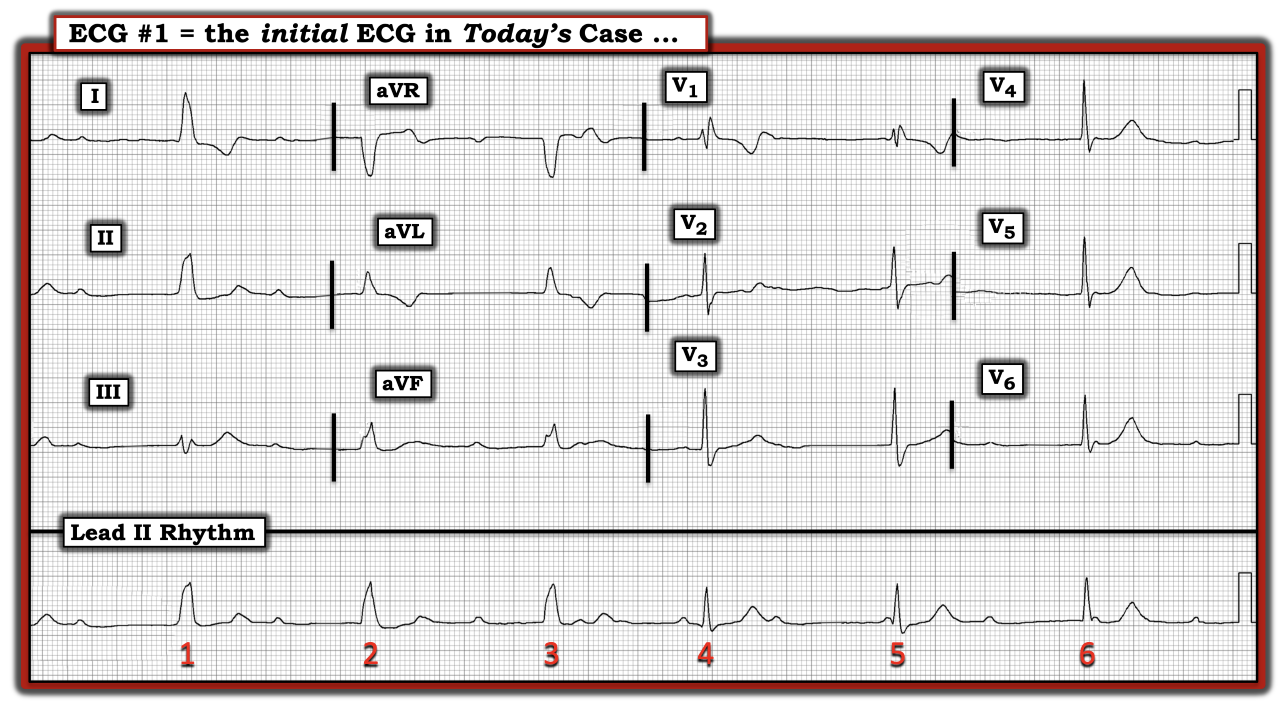
The rhythm in this tracing is challenging and complex because of a changing QRS morphology and the uncertain relationship between P waves and neighboring QRS complexes. The first three beats in the long lead II rhythm strip show a regular wide QRS rhythm in the low 40s, with a constantly changing PR interval. It looks like the initial part of this rhythm begins with high-grade AV block. Notably, the atrial rhythm appears to be fairly regular throughout the entire long lead II rhythm strip. This relationship is easiest to establish using calipers, which suggests “on-time” P waves are hidden within the QRS complex of beats 1 and 2, but otherwise can be “walked out” at a fairly regular P-P interval.
The key to interpreting this rhythm lies with beat 4, which clearly occurs earlier than expected, and which is preceded by a seemingly normal PR interval. This strongly suggests beat 4 is sinus-conducted. Note the appearance of beat 4 in simultaneously recorded leads V1, V2, and V3. This suggests beat 4 is conducted with a right bundle branch block (RBBB) pattern. QRS morphology of beats 5 and 6 in the long lead II rhythm strip is similar to the QRS morphology of beat 4 that we know is conducted. However, the P wave preceding beat 5 is too short to conduct, and no P wave at all precedes beat 6. This strongly suggests beats 5 and 6 are junctional escape beats that conduct with RBBB.
It is difficult to be certain of the etiology of this rhythm from this single strip. That said, although there is evidence of second-degree AV block (from the wide QRS and changing PR interval before the first three beats), the degree of AV block is not complete because beat 4 is sinus-conducted. The site of the escape focus for beats 1, 2, and 3 most likely is at the level of the ventricles. A second escape focus appears to be present at a higher level within the AV nodal conducting system, as beats 5 and 6 represent junctional escape beats that conduct with RBBB. Whether a pacemaker will be needed for this patient will depend on correlation with the overall clinical situation.
For more information about and further discussion of this case, please click here.
The ECG in the figure is from a woman who complained she had been experiencing chest pain for several days. What is the rhythm? Is there complete AV block?
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.