By Ken Grauer, MD
You are given the electrocardiogram (ECG) in the figure and told that the patient is a young man in his 20s who presents with acute dyspnea. The physical exam is remarkable for tachypnea, cyanosis, and clubbing of the extremities.
- How would you interpret the rhythm?
- Do the noted physical exam findings help in your assessment of the rhythm?
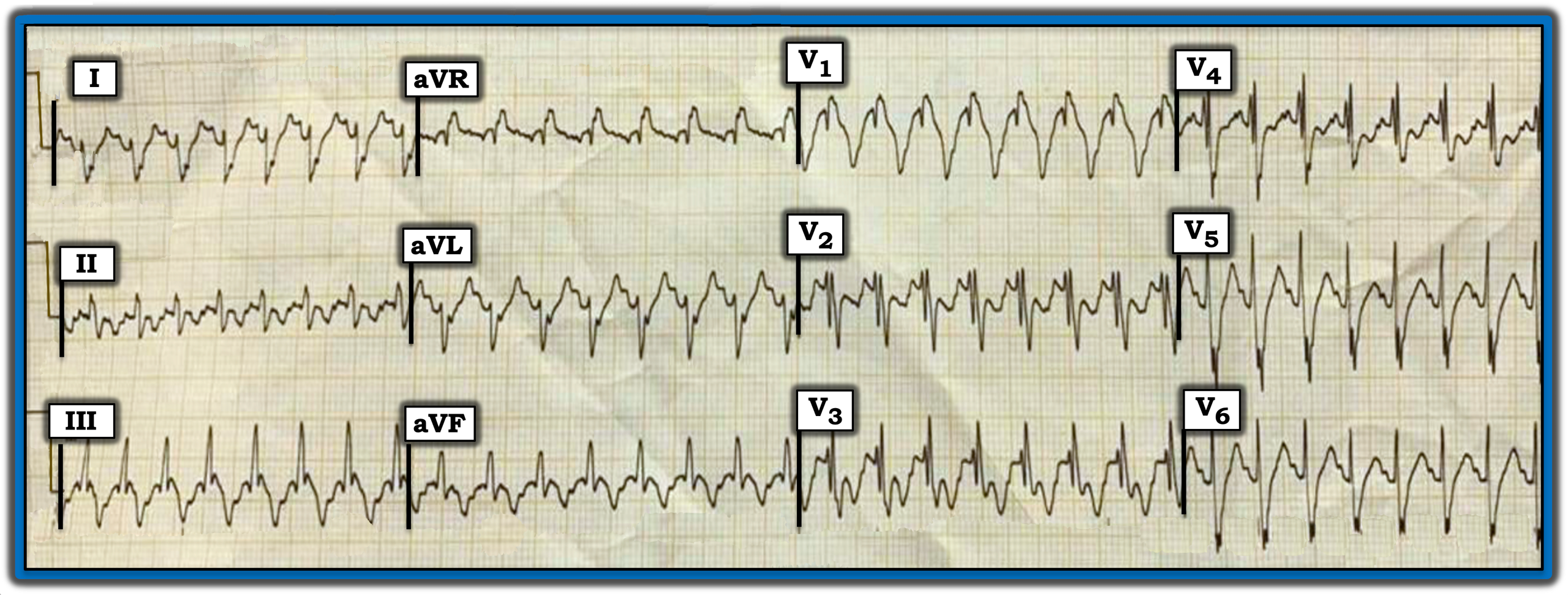
Interpretation: The 12-lead ECG in the figure shows a regular wide-complex tachycardia (WCT) at a rate of ~190 beats/minute without clear sign of sinus P waves.
- Statistically, most patients who present for emergency care with a regular WCT rhythm without a clear sign of sinus P waves will be in ventricular tachycardia (VT).
- That said, the QRS morphology of today’s rhythm potentially is consistent with right bundle branch block (RBBB) conduction because there is a predominantly positive QRS in lead V1 together with wide terminal S waves in lateral leads I and V6. In addition, the predominant negativity with straightened and steep descent of the S wave in lead I potentially is consistent with left posterior hemiblock (LPHB) conduction. This QRS morphology, which is potentially consistent with RBBB/LPHB conduction, suggests that today’s rhythm may be supraventricular.
- An additional finding regarding QRS morphology in favor of this WCT rhythm being supraventricular (with either preexisting bundle branch block or rate-
related aberrant conduction) is how narrow the initial R waves are in leads I, aVL, V5, and V6. VT typically arises outside the conduction system, which is why the initial QRS deflection tends to be wider (representing slower initial conduction).
The physical exam in today’s case helped interpret this rhythm.
- The fact that today’s patient is a young man with cyanosis and clubbing of the extremities suggests that, rather than a first presentation of idiopathic VT in a young man without underlying heart disease, the patient has some form of longstanding cardiac disorder that, over a period of years, has resulted in cyanosis and clubbing.
- In view of the clinical presentation, in association with ECG findings resembling RBBB/LBBB conduction with a narrow initial R wave deflection in all lateral leads, I suspected that this WCT rhythm was most likely supraventricular.
Follow-Up: Synchronized cardioversion restored sinus rhythm.
- QRS morphology in the post-conversion ECG resembled QRS morphology during the tachycardia. This confirmed that the regular WCT rhythm was indeed supraventricular and that this patient had a markedly abnormal baseline ECG for a man in his 20s. The patient turned out to have adult expression of a complex form of congenital heart disease.
Note: For more information about this case, visit https://tinyurl.com/KG-Blog-422.
You are given the electrocardiogram (ECG) in the figure and told that the patient is a young man in his 20s who presents with acute dyspnea. The physical exam is remarkable for tachypnea, cyanosis, and clubbing of the extremities. How would you interpret the rhythm? Do the noted physical exam findings help in your assessment of the rhythm?
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.