AUTHORS
C.S. Solomon, BSPharm, RPh, CTTS, NCTTP, Clinical Associate Professor, Department of Internal Medicine and Neurology, Wright State University Boonshoft School
of Medicine, Dayton, OH
Glen D. Solomon, MD, MACP, FRCP (London), Chairman, Department of Internal Medicine and Neurology, Wright State University Boonshoft School
of Medicine, Dayton, OH
WSU-BSOM COVID-19 Education Task Force Members, Wright State University Boonshoft School of Medicine, Dayton, OH
PEER REVIEWER
Sary Beidas, MD, MBI, FACP, Associate Professor of Medicine, Florida State University, Sarasota, FL
EXECUTIVE SUMMARY
During the COVID-19 pandemic, one medical school initiated a task force to bring together answers to common questions by clinicians and the public regarding the pandemic. This issue summarizes the results of that effort and is presented in a different format, with references included for each section.
For more than two years, we have been struggling with finding the right answers to a host of issues that are changing constantly in complexity and applicability.
- What should primary care physicians do if a patient tests positive?
- Why is it so difficult to interpret the medical literature in the face of often contradictory and politically charged theater?
- Where are the trusted sources of information?
- How should we respond to new, mutated viral strains? How do we decide on appropriate therapy for individual patients, and how do we prepare for the apparently inevitable next wave of infection?
Introduction
To disseminate accurate information effectively in our local community, a task force was formed inside Wright State University Boonshoft School of Medicine to educate clinicians and answer community members’ questions, first about vaccines, and second about all things COVID-19. More than 25 members, from faculty experts to medical students, have spent two and a half years providing community outreach, setting up at farmers’ markets, and hosting symposia for regional clinicians needing timely information about new vaccines. Through many phases of the COVID-19 pandemic, clinicians have needed to stay current with concepts of the virus, its variants, the changing methods of management and treatment, and best practices for patient benefit. Following are examples of some of our current questions.
What do I do if I test positive for COVID-19?
If a COVID-19 test (either a home test or a polymerase chain reaction [PCR] test) shows a positive result, the patient should isolate at home in a room separate from others, if possible, for at least five days. The first day of symptoms is day 0 (if asymptomatic, the day of the positive test is day 0). An N95 mask is the most suitable should the patient need to leave home or need to share bathrooms or other home areas. If the patient is a child, one adult should be assigned to care for the child. Day 5 is not the “definitive” day for no longer being contagious, according to the Centers for Disease Control and Prevention (CDC). With testing used as an important tool here, if the patient is antigen-positive, they may be infectious. Isolation can end if the patient is fever-free for 24 hours without the use of a fever-reducing medication and other symptoms are improving. Loss of taste and smell may persist longer and need not delay the end of isolation. The individual should continue to wear a well-fitted mask around others at home and in public for an additional five days after ending the isolation period.1
Why isn’t COVID-19 going away?
The extremely contagious nature of the currently most dominant coronavirus strains, the Omicron subvariants BA.4 and BA.5, which make up a combined 70% of coronavirus variants in the Unites States as of July 2, 2022, forces us to reexamine all we are doing as we try to live our daily lives.2 Since viruses have a goal of reproducing, variants are created with two purposes: to effectively infect the host (humans) and to evade the immune system. Because these subvariants are better able to evade the immune system, people may need to rethink the level of protection they choose. The benefits of being up to date with CDC vaccination recommendations is critical, meaning that the primary vaccination series is given and all available recommended boosters have been administered based on age and vulnerability. Updated COVID-19 boosters with Omicron adaptations or others, when available, may be more helpful than just additional doses of current COVID-19 vaccines. The Food and Drug Administration (FDA) now recommends that COVID-19 vaccine producers include components tailored to combat BA.4 and BA.5 for fall 2022 boosters. Properly fitted masks, although not mandated, should be employed as a precaution when one is in a vulnerable situation, whether it be at a grocery store or in a large group situation, along with social distancing and hand hygiene.3 Fitness centers, bars, offices, and long-term care facilities all are vulnerable places for people to be exposed to the virus.
Why is it so difficult to interpret the COVID-19 medical literature?
As a novel disease with global reach, there were more than a quarter-million medical research papers on COVID-19 published in the last two years. To expedite the sharing of information, some of these papers were released prior to peer review (“pre-print”). Additionally, because of the multiple waves of variants, the changing scope of vaccinations, and the differing populations and medical standards in other countries, it is challenging to compare studies. In reviewing the medical literature, it is critical to know when patients were enrolled (and which variant was predominant), their vaccination status (which vaccine and how many doses), and their demographics (years of age and underlying conditions).
Are there terms that will help me better interpret and explain information about COVID-19?
See Table 1 for terminology relating to COVID-19. This table provides the scientific definition for each term, a more colloquial interpretation, and an example providing context for the terminology. The interpretations were provided by members of the Wright State University Boonshoft School of Medicine COVID-19 Education Task Force.
Table 1. Common Epidemiologic Terms | |||
Term | Definition | COVID-19 Colloquial Interpretation | Example |
Prevalence | Proportion of persons who have a condition at or during a particular time period | Number of people who currently have COVID-19 | “The prevalence of COVID-19 is dropping; now, we have only 3,000 active cases across the state.” |
Incidence | Proportion or rate of persons who develop a condition during a particular time period | New COVID-19 cases in a given time | “The incidence of COVID-19 increased to 1,000 new cases per day.” |
Sensitivity | A test’s ability to correctly detect ill patients who have the condition | If you have COVID-19, this is the accuracy of a COVID-19 test to confirm you have COVID-19 | “The PCR test has a sensitivity of 98%; if it says you are COVID-19-positive, you probably are.” |
Specificity | A test’s ability to correctly reject healthy patients without a condition | If you do not have COVID-19, this is the accuracy of a COVID-19 test to confirm you do not have COVID-19 | “Using a saliva COVID-19 test is 98% specific; if it says you do not have COVID-19, you can trust it is probably right.” |
R0 (R-naught) | Expected number of secondary cases produced by a single infection in a completely susceptible population | If you have COVID-19, the number of people you will infect | “The Delta variant of COVID-19 had an R0 of about 5, so if you got COVID-19, you would probably give it to five people.” |
Case Fatality Rate | Proportion of people who die from a specified disease among all individuals diagnosed with the disease over a certain period of time | If someone gets COVID-19, how likely they are to die from it | “The case fatality rate for the Delta variant was 5%, which means if you get this variant of COVID-19, you are more likely to die from it than from the original COVID-19.” |
Sources: Infectious Diseases Society of America. IDSA guidelines on the diagnosis of COVID-19: Molecular diagnostic testing. Last updated Dec. 23, 2020. https://www.idsociety.org/practice-guideline/covid-19-guideline-diagnostics/ Warsi I, Khurshid Z, Shazam H, et al. Saliva exhibits high sensitivity and specificity for the detection of SARS-COV-2. Diseases 2021;9:38. Liu Y, Rocklöv J. The reproductive number of the Delta variant of SARS-CoV-2 is far higher compared to the ancestral SARS-CoV-2 virus. J Travel Med 2021;28:taab124. Murata GH, Murata AE, Perkins DJ, et al. Sustained beneficial effects of vaccination on the case fatality rate for COVID-19 infections. medRxiv 2022; Mar 14. doi: https://doi.org/10.1101/2022.01.22.22269689. [Preprint]. | |||
What are some of the most helpful resources when searching for COVID-19 information?
Part of the charge of the task force has been to develop a reliable toolkit of references and resources for physicians and other clinicians to use in answering patient questions about COVID-19.
Easily referenced resources on COVID-19 are essential for healthcare professionals in speaking with patients. Easy-to-navigate, dependable, up-to-date sources of information help serve patients requiring specific and timely answers to questions. Having a “go-to” list of resources can reduce confusion about COVID-19, making vaccination updates and other conversations more productive. Reliability can be determined by checking the source, author, and content.
Reliable sources include governmental agencies and reputable medical institutions. Medical organizations also can be effective resources:
- CDC: www.cdc.gov
- Johns Hopkins Medicine: www.hopkinsmedicine.org (for COVID-19 information and updates)
- COVID.gov (for a general COVID-19 toolkit)
- American Academy of Pediatrics: www.aap.org
- Infectious Diseases Society of America: www.idsociety.org
- American College of Physicians: www.acponline.org
- American Pharmacists Association: www.pharmacist.com
- University of Liverpool COVID-19 Drug Interactions: www.covid19-druginteractions.org/checker
Recommended for ease of use: The Public Health Communications Collaborative (https://publichealthcollaborative.org) is a resource initiated in August 2020 as a result of rapidly changing information concerning COVID-19.4 The platform was founded by the CDC and others to combine and organize answers to questions commonly asked by patients of providers. The format of this platform allows for easy access to commonly asked questions, along with shareable graphics and webinars that can be accessed by all.
A unique and up-to-date resource: We Can Do This (https://wecandothis.hhs.gov), a platform created by the U.S. Department of Health and Human Services, provides more than 600 resources to answer specific questions for different patient populations.5 Increasing community confidence and COVID-19 education, this platform covers topics ranging from vaccination during pregnancy to booster recommendations in those 50 years of age and older.
A dependable source: Boosting COVID-19 Vaccine Confidence (https://primeinc.org/online/boosting-covid-19-vaccine-confidence-educational-toolkit-providers) is an educational toolkit for providers, created by PRIME.6 This interactive educational format allows providers to gain confidence in speaking with patients about the benefits and risks of vaccination. By including a full description of what COVID-19 is and how the vaccines work, this platform breaks down the pandemic in an easy-to-explain manner. This patient-friendly toolkit and training session allows for both providers and patients to better understand why vaccines are important.
Recommended for accuracy: COVID-19 Toolkits (https://www.cdc.gov/coronavirus/2019-ncov/communication/toolkits/index.html) is a resource provided by the CDC that offers accurate and relevant information on COVID-19 vaccines, boosters, masks, and indications for different populations.7 This source allows providers to access the latest guidelines and recommendations concerning COVID-19. Additionally, it also includes contact tracing recommendations, which can be especially helpful in school and long-term care facility populations, through the health department.
Since COVID-19 constantly is shaping healthcare in new ways, the task force thought it imperative to formulate an educational toolkit for both community members and healthcare providers.8 By consistently updating the toolkit with the latest resources and guidelines, misinformation and anxiety related to COVID-19 can be reduced within the community. Resources that allow healthcare providers to gain confidence in their knowledge and understanding of COVID-19 are included. During a pandemic, it is important for providers to have the latest information available to aid patients in making the best decisions for themselves. By using toolkits that are updated continually, healthcare providers have organized, reliable resources.
References
- Centers for Disease Control and Prevention. Quarantine and isolation. Updated March 30, 2022. https://www.cdc.gov/coronavirus/2019-ncov/your-health/quarantine-isolation.html
- Centers for Disease Control and Prevention. Variant proportions. https://covid.cdc.gov/covid-data-tracker/#variant-proportions
- Centers for Disease Control and Prevention. How to protect yourself & others. Updated Feb. 25, 2022. https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/prevention.html
- Public Health Communications Collaborative. Communications resources for public health officials. Published March 7, 2022. https://publichealthcollaborative.org
- We Can Do This. COVID-19 public education campaign. Published April 4, 2022. https://wecandothis.hhs.gov
- PRIME. Recommended free CME and other online educational activities. Published Sept. 15, 2021. https://primeinc.org/online
- Centers for Disease Control and Prevention. COVID-19 toolkits. Updated April 11, 2022. https://www.cdc.gov/coronavirus/2019-ncov/communication/toolkits/index.html
- Wright State University Boonshoft School of Medicine. COVID-19 vaccine resources. Published March 8, 2021. https://medicine.wright.edu/about/news-and-events/article/covid-19-vaccine-resources
Symptoms of COVID-19
What are the presenting symptoms of COVID-19, and which patients are at high risk for a poor outcome?
Symptoms of COVID-19 are cough, fever, chills, difficulty breathing, body aches, sore throat, loss of taste or smell, diarrhea, headache, fatigue, nausea/vomiting, and/or congestion/runny nose.1 Patients who are concerned they may have COVID-19 should reach out to their provider as soon as possible. See Table 2 for common conditions associated with poor outcomes and more severe COVID-19, including hospitalization, intensive care, ventilator use, and death.
Table 2. Common Conditions Associated with Poor Outcomes and More Severe COVID-192-13 |
|
Many COVID-19 precautions are being lifted, causing one to ask, “Is being out in the community safe? Am I at risk of developing severe symptoms? Am I part of the high-risk population?” Higher risk patients, including racial and ethnic minorities, should be advised to use properly fitted masks, social distance, avoid poorly ventilated areas and large gatherings, and stay up to date with all CDC recommended vaccinations.14,15 COVID.gov is a patient-friendly website, and test to treat locations can be found at 1-800-232-0233 (TTY: 1-888-720-7489).16
References
- Johns Hopkins Medicine. COVID-19 vs. the flu. Updated Feb. 23, 2022. https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/coronavirus-disease-2019-vs-the-flu
- Centers for Disease Control and Prevention. People with certain medical conditions. Updated May 2, 2022. https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html#obesity
- Robilotti EV, Babady NE, Mead PA, et al. Determinants of COVID-19 disease severity in patients with cancer. Nat Med 2020;26:1218-1223.
- Mayo Clinic. COVID-19: Who’s at higher risk of serious symptoms? https://www.mayoclinic.org/diseases-conditions/coronavirus/in-depth/coronavirus-who-is-at-risk/art-20483301
- National Institutes of Health COVID-19 Treatment Guidelines. Special
considerations in people with HIV. Updated May 2, 2022. https://www.covid19treatmentguidelines.nih.gov/special-populations/hiv/ - National Institutes of Health COVID-19 Treatment Guidelines. Special considerations in pregnancy. Updated July 8, 2021. https://www.covid19treatmentguidelines.nih.gov/special-populations/pregnancy/
- Johns Hopkins Medicine. Who is at higher risk for severe coronavirus disease? Updated Dec. 8, 2021. https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/coronavirus-and-covid19-who-is-at-higher-risk
- Gupta R, Ghosh A, Singh AK, Misra A. Clinical considerations for patients with diabetes in times of COVID-19 epidemic. Diabetes Metab Syndr 2020;14:211-212.
- Panepinto JA, Brandow A, Mucalo L, et al. Coronavirus disease among persons with sickle cell disease, United States, March 20-May 21, 2020. Emerg Infect Dis 2020;26:2473-2476.
- Dard R, Janel N, Vialard F. COVID-19 and Down’s syndrome: Are we heading for a disaster? Eur J Hum Genet 2020;28:1477-1478.
- Gao C, Cai Y, Zhang K, et al. Association of hypertension and antihypertensive treatment with COVID-19 mortality: A retrospective observational study. Eur Heart J 2020;41:2058-2066.
- Frydrych LM, Bian G, O’Lone DE, et al. Obesity and type 2 diabetes mellitus drive immune dysfunction, infection development, and sepsis mortality. J Leukoc Biol 2018;104:525-534.
- Muniyappa R, Gubbi S. COVID-19 pandemic, coronaviruses, and diabetes mellitus. Am J Physiol Endocrinol Metab 2020;318:E736-E741.
- Centers for Disease Control and Prevention. Obesity, Race/Ethnicity, and COVID-19. Last reviewed May 20, 2022. https://www.cdc.gov/obesity/data/obesity-and-covid-19.html
- Centers for Disease Control and Prevention. How to protect yourself & others. Updated Feb. 25, 2022. https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/prevention.html
- Office of the Assistant Secretary for Preparedness and Response. Test to Treat. https://aspr.hhs.gov/TestToTreat/Pages/default.aspx
Public Health Challenges
What are some of the public health challenges related to COVID-19?
In 2020, the COVID-19 pandemic radically changed our approach to public health. Before the COVID-19 pandemic, most people would have assumed that young, healthy, immunocompetent individuals would be resistant to all but the most severe infectious diseases; meanwhile, only older individuals or those with preexisting conditions would be considered at risk of severe negative outcomes from less virulent endemic diseases, such as influenza. Unlike expectations from previous experience, young, healthy people; asymptomatic people; and people not considered high-risk may be affected negatively by COVID-19.
The goal of increasing access and education related to COVID-19 vaccines was discussed as part of a recent Journal of the American Medical Association (JAMA) Network Health Agencies Update. An administrator stated that investments in community-based funding help reduce disparities in underserved communities disproportionately affected by the pandemic.
The high infectivity of COVID-19, combined with its potential for severe disease, has ignited a new focus on the relationship between immunology and pathologic processes. Research suggests that various biopsychosocial factors and health behaviors can predispose people to COVID-19.1
During this pandemic, social distancing has remained a prime approach to preventing infection with COVID-19. However, conflicting perspectives around the severity of COVID-19 have caused discussions regarding prevention to become more political than public health-focused. Current research has identified specific barriers, such as socioeconomic status, occupation, and housing density as major obstacles to proper social distancing.2,3 Essential workers, unhoused individuals, and minority populations are groups of interest when thinking about disparities in COVID-19 infection.4
Eradication of COVID-19 is unlikely, since its causative viral agent continues to mutate, which is common for all ribonucleic acid (RNA) viruses. Geographic separation of exposures tends to result in genetically distinct variants.5 Although social distancing is an effective method for preventing the spread of COVID-19, it is most effective as part of a larger prevention strategy that includes good sanitation practices, mask wearing, and vaccine adherence.6 Historically, vaccines have been an excellent tool in the control and eradication of disease. Although many people were thrilled to have such an option for COVID-19, others noted significant concerns about the speed of vaccine development, inconsistency in messaging from public health officials, and the potential for adverse outcomes.7
There are considerable differences in COVID-19 vaccine uptake among different populations, ranging from distrust of the medical establishment to reduced access to vaccines. Healthcare inequities, personal opinions valuing or devaluing vaccine access, and misinformation contribute to achieving public health goals. Initially, people of color had lower vaccination rates. Data from the Centers for Disease Control and Prevention (CDC), in the April 2022 Kaiser Family Foundation Report, show that 77% of the total U.S. population had received at least one dose of a COVID-19 vaccine. With unvaccinated people at increased risk of infection, severe illness, and death, white people accounted for two-thirds (64%) of people who remain unvaccinated.8 With booster shot eligibility now expanding to many of the pediatric groups, ensuring equity in uptake of boosters and primary vaccinations among children will continue to be a top priority.
References
- Gonzales A, Lee EC, Grigorescu V, et al. Overview of barriers and facilitators in COVID-19 vaccine outreach. Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services. Published Sept. 13, 2021. https://aspe.hhs.gov/reports/covid-19-vaccine-outreach
- Garnier R, Benetka JR, Kraemer J, Bansal S. Socio-economic disparities in social distancing during the COVID-19 pandemic in the United States. medRxiv 2020; Nov 9. doi.org/10.1101/2020.11.07.20201335. [Preprint].
- Bibbins-Domingo K. This time must be different: Disparities during the COVID-19 pandemic. Ann Intern Med 2020;173:233-234.
- Centers for Disease Control and Prevention. Risk of exposure to COVID-19. Updated Dec. 10, 2020. https://www.cdc.gov/coronavirus/2019-ncov/community/health-equity/racial-ethnic-disparities/increased-risk-exposure.html#ref10
- Bollinger R, Ray S, Maragakis L. COVID variants: What you should know. Johns Hopkins Medicine. Updated April 8, 2022. https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/a-new-strain-of-coronavirus-what-you-should-know#:~:text=Alpha%2C%20beta%2C%20gamma%2C%20delta,2%20variants%20of%20high%20consequence
- Su Z, Wen J, McDonnell D, et al. Vaccines are not yet a silver bullet: The imperative of continued communication about the importance of COVID-19 safety measures. Brain Behav Immun Health 2021;12:100204.
- Troiano G, Nardi A. Vaccine hesitancy in the era of COVID-19. Public Health 2021;194:245-251.
- Centers for Disease Control and Prevention. COVID Data Tracker. https://covid.cdc.gov/covid-data-tracker
Prevention of COVID-19
What can my family do to prevent getting COVID-19?
Our understanding of COVID-19 has grown rapidly since the start of the pandemic and, in turn, our management of the disease has become more effective and standardized. Despite these advances, COVID-19 still is a potentially deadly virus. Prevention, rather than treatment, is the goal. Here, we discuss views on physical mitigation and vaccines as preventive measures.
COVID-19 is a respiratory virus that spreads when an infected person breathes out droplets and very small particles that contain the virus via airborne transmission, such as breathing or speaking. Some of these droplets are large and fall to the ground rather quickly, while others are smaller particles or aerosols (less than 10 microns in diameter) and can linger in the air.1 These droplets and particles can be breathed in by other people or land in their eyes, nose, or mouth.2 Masking acts as a barrier, helping to block droplets and even some aerosols.1,3 The ability to filtrate particles and droplets varies based on characteristics, such as the type of material, the number of layers of material, and the fit. However, even simple cloth masks can block some droplets and aerosols. Numerous studies have shown that masks are effective in helping to reduce the spread of infection.1,3
Patients should be encouraged to wear masks when out in public, both to reduce their risk of contracting SARS-CoV-2 as well as to reduce their risk of potentially spreading an asymptomatic or pre-symptomatic infection.
Practicing social distancing, using telecommunication instead of in-person contact, physical distancing at social events, staying at least six feet from others, or staying away from large gatherings helps prevent the spread of COVID-19.2 Proactive use of testing to detect either SARS-CoV-2 or biomarkers of SARS-CoV-2, or antibodies made after getting COVID-19, prior to such activities can help refine and reduce superspreader opportunities in schools and elsewhere.
Vaccines are another important tool in the fight against COVID-19. In resource-rich countries, such as the United States, COVID-19 has become a vaccine-preventable disease. This term does not reflect that a vaccine will eradicate all diseases for which there is a vaccine, but instead represents that the disease can be rendered less deadly and less severe through vaccination. Vaccine-preventable diseases can cause long-term illness, hospitalization, and death.4
Despite increasing numbers of vaccinated individuals becoming infected with the extremely contagious Omicron variant, vaccines have remained highly effective at preventing hospitalizations and death.5 Studies also have shown that keeping vaccinations up to date helps enhance the patient’s immune response and improve protection against COVID-19.5 All eligible patients should be up to date with all CDC-recommended vaccinations to maximize prevention of infection, hospitalization, and death. (For current vaccine information for specific patients, see toolkit references.)
Although life in many areas of the United States is regaining elements of pre-COVID normalcy, it is important that we use information and resources to prevent further morbidity and mortality.6,7
References
- Brooks JT, Butler JC. Effectiveness of mask wearing to control community spread of SARS-CoV-2. JAMA 2021;325:998-999.
- Centers for Disease Control and Prevention. How COVID-19 spreads. Updated July 14, 2021. https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/how-covid-spreads.html
- Centers for Disease Control and Prevention. Science Brief: Community use of masks to control the spread of SARS-CoV-2. Updated Dec. 6, 2021. https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/masking-science-sars-cov2.html
- Centers for Disease Control and Prevention. Vaccines and preventable diseases. Last reviewed Nov. 22, 2016. www.cdc.gov/vaccines/vpd/index.html
- Centers for Disease Control and Prevention. Science Brief: Omicron (B.1.1.529) variant. Updated Dec. 2, 2021. https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/scientific-brief-omicron-variant.html
- Centers for Disease Control and Prevention. COVID Data Tracker. April 2022. https://covid.cdc.gov/covid-data-tracker/#datatracker-home
- World Health Organization. WHO Coronavirus (COVID 19) Dashboard. April 2022. https://covid19.who.int/
Pregnancy and COVID-19
Does COVID-19 vaccination or COVID-19 infection affect pregnancy?
Pregnancy or recent pregnancy is associated with a higher risk for severe COVID-19.1 COVID-19 also is associated with a higher risk of numerous prenatal and perinatal complications, including preeclampsia, maternal mortality, and preterm birth.2,3 Pregnant people with additional comorbidities, such as advanced maternal age, high body mass index (BMI), preexisting diabetes, or chronic hypertension, also are associated with a higher risk for intensive care unit (ICU) admission or forced ventilation.2,3 Despite the increased risk associated with pregnancy and COVID-19 infections, vaccination coverage and uptake among pregnant people remains low.4,5 The pregnant population provides opportunity for better education and promotion of both the vaccines and COVID-19 prevention strategies.
Two additional questions related to pregnancy are whether the vaccine is safe for both mother and fetus and whether vaccination during pregnancy is safe and beneficial to the newborn.6,7 Studies of pregnant persons have shown no increased pregnancy-related adverse effects from COVID-19 vaccination, nor increased risk of miscarriage.6,8,9 A helpful counseling point for patients considering vaccination is that immunization likely will help protect their child against COVID-19 by the passing of anti-spike protein immunoglobulin G (IgG) antibodies through the placenta. It has been found, in mothers who were vaccinated between 20 and 32 weeks of gestation, that detectable levels of anti-spike IgG antibodies were found in 98% of their infants at two months, with that number dropping to 57% at six months (compared to only 8% of infants with detectable IgG whose mothers were infected with COVID-19 during the same time period).7
The American College of Obstetricians and Gynecologists (ACOG) and the CDC guidelines recommend vaccination any time before or during pregnancy, including for those planning to become pregnant, those who are pregnant, or those who are breastfeeding to provide some immunity to their babies.10
Education on vaccine safety and efficacy, along with proper COVID-19 prevention strategies, such as masking and social distancing, are a critical responsibility of primary care physicians. A poll of 12,887 people indicated that primary care providers were the most trusted source of information about the COVID-19 vaccine and the most preferred place to get vaccinated.11 The low levels of vaccination in pregnant populations, the increased risk of complications during pregnancy from COVID-19, and the additional benefits to the fetus from maternal vaccination highlight an opportunity to effect a positive change through proper education and health promotion with pregnant patients.
References
- Centers for Disease Control and Prevention. Science Brief: Evidence used to update the list of underlying medical conditions associated with higher risk for severe COVID-19. Updated Feb. 15, 2022. https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/underlying-evidence-table.html
- Allotey J, Stallings E, Bonet M, et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: Living systematic review and meta-analysis. BMJ 2020;370:m3320.
- Villar J, Ariff S, Gunier RB, et al. Maternal and neonatal morbidity and mortality among pregnant women with and without COVID-19 infection: The INTERCOVID Multinational Cohort Study. JAMA Pediatr 2021;175:817-826.
- Blakeway H, Prasad S, Kalafat E, et al. COVID-19 vaccination during pregnancy: Coverage and safety. Am J Obstet Gynecol 2022;226:236.e1-236.e14.
- Stock SJ, Carruthers J, Calvert C, et al. SARS-CoV-2 infection and COVID-19 vaccination rates in pregnant women in Scotland. Nat Med 2022;28:504-512.
- Shimabukuro TT, Kim SY, Myers TR, et al. Preliminary findings of mRNA Covid-19 vaccine safety in pregnant persons. N Engl J Med 2021;384:2273-2282.
- Shook LL, Atyeo CG, Yonker LM, et al. Durability of anti-spike antibodies in infants after maternal COVID-19 vaccination or natural infection. JAMA 2022;327:1087-1089.
- Magnus MC, Gjessing HK, Eide HN, et al. Covid-19 vaccination during pregnancy and first-trimester miscarriage. N Engl J Med 2021;385:2008-2010.
- Kharbanda EO, Haapala J, Desilva M, et al. Spontaneous abortion following COVID-19 vaccination during pregnancy. JAMA 2021;326:1629-1631.
- Centers for Disease Control and Prevention. COVID-19 vaccines while pregnant or breastfeeding. Updated June 13, 2022. https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/pregnancy.html
- African American Research Collaborative. American COVID-19 Vaccine Poll. https://covidvaccinepoll.com
Fertility and COVID-19
Does COVID-19 vaccination or COVID-19 infection affect infertility?
Various viral infections are associated with impaired male fertility and decreased semen quality.1 The most well-known of these viruses is mumps, but also includes hepatitis B and C, as well as human papillomavirus (HPV).1 Most recently there is evidence that infection with SARS-CoV-2, especially moderate to severe infection, has been linked with impairments to male fertility.1
SARS-CoV-2 has been found to infect cells by binding to the angiotensin-converting enzyme 2 (ACE-2) receptor on the cell surface.1-3 The receptor can be found on up to 72 different types of tissue in the human body, including the heart, lung, brain, and testis.2 After gaining entry into the cell, viral replication begins to occur, leading to cellular dysfunction. This triggers an inflammatory cascade of events involving multiple cytokines to prevent continued viral replication and infection of other cells that can end up damaging the body in the process.
It has been postulated that male fertility is affected by SARS-CoV-2 infection through multiple different mechanisms, including direct damage to cells, with indirect damage from inflammation.2 In terms of direct effects, viral infection via ACE-2 receptors on the testis can lead to inflammatory changes in male reproductive interstitial tissue and infertility. Reduction of Sertoli and Leydig cells can lead to less testosterone, lack of nourishment of sperm, and, ultimately, impaired fertility.2 Indirectly, increased inflammation and cytokine storm following COVID-19 infection may induce a higher temperature of the testes with increased blood flow, leading to germ cell damage, ultimately jeopardizing the blood-testis barrier.3 This adversely affects spermatogenesis and hormone production within the testes.3 In addition, drugs, such as glucocorticoids and interferons used to treat SARS-CoV-2 infections, may be gonadotoxic, adversely affecting the male reproductive system.3
Concerning female infertility, results have been less conclusive regarding the long-term effects of SARS-CoV-2 infection. It has been noted that ACE-2 also is highly expressed in female reproductive tissues, including those of the ovaries, vagina, and uterus.4 Although there have been changes noted to the female menstrual cycle associated with COVID-19, it appears that this is a temporary response, possibly associated with the increased physiologic stress related to infection.4 Ovarian reserve did not seem to be significantly altered by COVID-19 infection, except in a few instances of noted severe infection.4
There is no current evidence that suggests COVID-19 vaccines affect fertility; rather, they should be considered as a possible modality to prevent infertility.
References
- Adamyan L, Elagin V, Vechorko V, et al. A review of recent studies on the effects of SARS-CoV-2 infection and SARS-CoV-2 vaccines on male reproductive health. Med Sci Monit 2022;28:e935879.
- Seymen CM. The other side of COVID-19 pandemic: Effects on male fertility J Med Virol 2021;93:1396-1402.
- Tian Y, Zhou LQ. Evaluating the impact of COVID-19 on male reproduction. Reproduction 2021;161:R37-R44.
- Carp-Veliscu A, Mehedintu C, Frincu F, et al. The effects of SARS-CoV-2 infection on female fertility: A review of the literature. Int J Environ Res Public Health 2022;19:984.
Vaccination vs. Naturally Acquired Immunity
If I already have had COVID-19, should I still be vaccinated?
Providers should encourage their previously infected patients to seek vaccination for COVID-19. Many patients infected with COVID-19, having not been vaccinated previously, may mistakenly believe they are equally protected from future reinfection by their natural immunity, compared to people already vaccinated. The duration of naturally acquired immunity differs by COVID-19 variant. Neutralizing antibodies after natural infection have a half-life of two to three months, while with messenger RNA (mRNA) vaccination, the half-life extends to three to six months.1 Both cellular and humoral immunity appears to be more durable after vaccination compared with infection. Studies have shown that vaccination, in combination with previous infection, reduces the frequency of reinfection.2,3 Individuals who have been both infected and vaccinated show a more robust immune response when compared to those who have naturally acquired immunity alone.4,5 Additionally, patients who have been infected previously with COVID-19 generate a stronger immune response from vaccination, compared with vaccinated individuals who have not been infected previously.6,7
Many studies have estimated that previous infection plus an mRNA vaccine dose produces an antibody response similar to two doses of vaccine in a person without a history of infection.1 Antibodies induced by vaccination have been shown to be more diverse and have greater reactivity against variants than antibodies from prior infection.8 Multiple studies have shown varying rates of seronegativity following confirmed COVID-19 infection, further suggesting that natural infection does not guarantee immunity.9-12 Patients with lower viral loads and less symptomatic disease were more likely to lack seroconversion and, conversely, severe disease did not guarantee a seroconversion.13 Vaccination against the SARS-CoV-2 virus after previous infection may amplify the immune response, provide broader protection against different strains of the virus, and provide protection to those who may have had an absent or low level of immunity created by natural infection.
References
- Centers for Disease Control and Prevention. Science Brief: SARS-CoV-2 infection-induced and vaccine-induced immunity. Updated Oct. 29, 2021. https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/vaccine-induced-immunity.html#anchor_1635540136596
- Cavanaugh AM, Spicer KB, Thoroughman D, et al. Reduced risk of reinfection with SARS-CoV-2 after COVID-19 vaccination – Kentucky, May-June 2021. MMWR Morb Mortal Wkly Rep 2021;70:1081-1083.
- Nordstrom P, Ballin M, Nordstrom A. Risk of SARS-CoV-2 reinfection and COVID-19 hospitalisation in individuals with natural and hybrid immunity: A retrospective, total population cohort study in Sweden. Lancet Infect Dis 2022;22:781-790.
- Hall V, Foulkes S, Insalata F, et al. Protection against SARS-CoV-2 after Covid-19 vaccination and previous infection. N Engl J Med 2022;386:1207-1220.
- Milne G, Hames T, Scotton C, et al. Does infection with or vaccination against SARS-CoV-2 lead to lasting immunity? Lancet Respir Med 2021;9:1450-1466.
- Bates TA, McBride SK, Leier HC, et al. Vaccination before or after SARS-CoV-2 infection leads to robust humoral response and antibodies that effectively neutralize variants. Sci Immunol 2022;7:eabn8014.
- Kent SJ, Juno JA. Vaccination after prior COVID-19 infection: Implications for dose sparing and booster shots. EBioMedicine 2021;72:103586.
- Castro Dopico X, Ols S, Loré K, Karlsson Hedestam GB. Immunity to SARS-CoV-2 induced by infection or vaccination. J Intern Med 2022;291:32-50.
- Wellinghausen N, Plonné D, Voss M, et al. SARS-CoV-2-IgG response is different in COVID-19 outpatients and asymptomatic contact persons. J Clin Virol 2020;130:104542.
- Thiruvengadam R, Chattopadhyay S, Mehdi F, et al. Longitudinal serology of SARS-CoV-2-infected individuals in India: A prospective cohort study. Am J Trop Med Hyg 2021;105:66-72.
- Masiá M, Telenti G, Fernández M, et al. SARS-CoV-2 seroconversion and viral clearance in patients hospitalized with COVID-19: Viral load predicts antibody response. Open Forum Infect Dis 2021;8:ofab005.
- Oved K, Olmer L, Shemer-Avni Y, et al. Multi-center nationwide comparison of seven serology assays reveals a SARS-CoV-2 non-responding seronegative subpopulation. EClinicalMedicine 2020;29:100651.
- Liu W, Russell RM, Bibollet-Ruche F, et al. Predictors of nonseroconversion after SARS-CoV-2 infection. Emerg Infect Dis 2021;27:2454-2458.
Treatment Strategies
What are some of the current treatment strategies for non-hospitalized COVID-19 patients?
Treatment of COVID-19 in outpatients generally is limited to patients at high risk of severe disease. Four available therapies are nirmatrelvir/ritonavir (Paxlovid), molnupiravir (Lagevrio), sotrovimab (Xevudy), and remdesivir (Veklury). Nirmatrelvir/ritonavir combination acts as an oral protease inhibitor. Used in patients with at least one risk factor for progression of disease, nirmatrelvir/ritonavir can be taken at home, lowering the risk of hospitalization by nearly 90%. Treatment needs to be started within five days of either the beginning of symptoms or a confirmed positive COVID-19 test. Because there are many potential drug interactions, drug reconciliation, with possible temporary therapeutic changes, is a necessity prior to dispensing the treatment.1 Patients with severe kidney or liver impairment should not be prescribed nirmatrelvir/ritonavir. Regimens of medications or dietary supplements significantly metabolized via cytochrome P450 enzyme reactions (see the University of Liverpool COVID-19 Drug Interactions resource at www.covid19-druginteractions.org/checker) must be thoroughly scrutinized for patient safety prior to prescription. The so-called “rebound effect,” recurrent symptoms or positive polymerase chain reaction (PCR) test occurring two to eight days post-nirmatrelvir/ritonavir treatment course, remains a concern. Recurring symptoms after completing the five-day course do not appear to represent reinfection or resistance to nirmatrelvir/ritonavir. Retreatment with nirmatrelvir/ritonavir is not recommended, nor is it part of the current emergency use authorization (EUA) for this medicine.
Sotrovimab is a monoclonal antibody given as a single infusion. It can be given within 10 days of symptom onset. Sotrovimab is not effective against the Omicron variant BA.2 and no longer is authorized for use in areas with high BA.2 frequency. Remdesivir injection was the first drug to receive FDA approval for use specifically in COVID-19. A prodrug of an adenosine analog, it is given once daily via intravenous infusion for up to 10 days.
Molnupiravir is an oral antiviral drug that works by preventing the SARS-CoV-2 virus from making more copies of itself. It appears to be less effective in preventing hospitalization and death than the other drugs, lowering the risk of hospitalization and death by about 30%. It is recommended for use only when the other three options are not available. It should be given within five days of symptom onset.
To improve access to these therapies, an online locator tool is available at https://covid-19-therapeutics-locator-dhhs.hub.arcgis.com.
For pre-exposure prophylaxis, the FDA has authorized, via EUA, the combination of tixagevimab plus cilgavimab (Evusheld). This is a long-acting anti-SARS-CoV-2 monoclonal antibody combination used for individuals who do not have SARS-CoV-2 infection and have not recently been exposed to an individual with SARS-CoV-2 infection, but who are at risk for inadequate immune response to COVID-19 vaccination or have a documented history of severe adverse reaction to an available COVID-19 vaccine or its components. It provides at least six months of protection. Information on each of these treatments can be found at:
- https://covid19treatmentguidelines.nih.gov/therapies/
- https://covid19treatmentguidelines.nih.gov/therapies/anti-sars-cov-2-antibody-products/anti-sars-cov-2-monoclonal-antibodies/
What is the role of dietary supplements in treating COVID-19 infections?
Recent studies have evaluated several dietary supplements in the treatment of COVID-19-infected patients. Dietary supplements, as regulated currently, are not considered as medicines, nor are they intended to treat, diagnose, mitigate, prevent, or cure disease. Although limited evidence exists about the safety and effectiveness of using vitamin D and zinc for treating or preventing COVID-19, several studies have been conducted to assess in vitro antiviral properties and how this might translate into humans.
Current literature shows that people receiving vitamin D and zinc, either individually or combined, had no improvement in symptoms, and no faster recovery or change in intubation status nor outcome.2 Many individuals who were infected by COVID-19 were found to have low levels of vitamin D.3 Despite supplementation with vitamin D during COVID-19 infection, there was no change in outcomes for these patients.2,3 Patients with normal vitamin D levels had more favorable outcomes than patients with low vitamin D levels.2 This suggests that patients who are deficient in vitamin D may have less favorable health outcomes after COVID-19 infection than patients who have normal serum levels of vitamin D. However, there is no evidence that patients with normal vitamin D serum levels benefit from vitamin D supplementation during active COVID-19 infection. There are potential risks to over-supplementing with vitamin D. Current studies found that overzealous dosing with vitamin D led to side effects, including nausea, vomiting, altered sensorium, constipation, headaches, acute kidney injury, weight loss, and symptomatic hypercalcemia.4 In summary, vitamin D does not appear to be beneficial as a treatment for COVID-19-infected patients.
Because zinc may play a role in the immune response, it has been studied in COVID-19 patients.2 A recent meta-analysis of patients supplemented with zinc during active COVID-19 infection showed no evidence of benefit to patients.2 There is evidence that supra-physiologic supplementation with zinc may lead to irreversible loss of taste and smell.3 Because COVID-19 symptoms can include loss of taste and smell, zinc supplementation may cause providers a challenge in differentiating between COVID-19 symptoms and effects from consuming zinc.
Deficiencies of vitamin D and/or zinc have been associated with less favorable outcomes in COVID-19 patients.2,4 Neither supplementing vitamin D and/or zinc during a COVID-19 infection, nor treating low levels of either, has shown improved outcomes. Other supplements also have failed to show positive outcomes in COVID-19.
References
- National Institutes of Health. Ritonavir-boosted nirmatrelvir (Paxlovid). Updated May 13, 2022. https://www.covid19treatmentguidelines.nih.gov/therapies/antiviral-therapy/ritonavir-boosted-nirmatrelvir--paxlovid-/
- Speakman LL, Michienzi SM, Badowski ME. Vitamins, supplements and COVID-19: A review of currently available evidence. Drugs Context 2021;10:2021-6-2.
- Joachimiak MP. Zinc against COVID-19? Symptom surveillance and deficiency risk groups. PLoS Negl Trop Dis 2021;15:e0008895.
- Kaur P, Mishra SK, Mithal A. Vitamin D toxicity resulting from overzealous correction of vitamin D deficiency. Clin Endocrinol (Oxf) 2015;83:327-331.
Long COVID
What is long COVID?
Because post-COVID-19 syndrome, also called long COVID or post-acute sequelae of COVID-19 (PASC), has no universal definition, it is difficult to compare studies. The World Health Organization (WHO) defines PASC as occurring in people with a history of probable or confirmed SARS-CoV-2 infection, usually within three months from the onset of COVID-19, with symptoms and effects lasting at least two months, unexplained by an alternative diagnosis.
Post-COVID-19 conditions are reported by individuals with both symptomatic and asymptomatic initial infection. Many people who experience mild or asymptomatic SARS-CoV-2 infections do not receive PCR or antigen testing at the time of acute infection, making it more challenging to attribute later symptoms to SARS-CoV-2 infection.1,2 Symptoms associated with post-COVID-19 conditions are heterogeneous and often non-specific, overlapping with many common medical conditions, and may be difficult to fully capture in any single data system.1,3,4 Long-term symptoms are common, occurring in one-quarter to one-half of all COVID-19 patients.
Commonly reported symptoms associated with long COVID are illustrated in Figure 1.
Figure 1. Long COVID Symptoms |
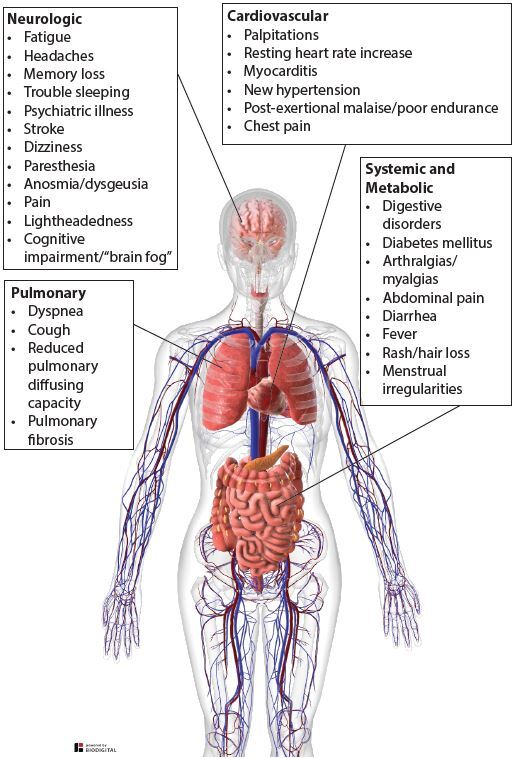 |
Sources: Centers for Disease Control and Prevention. Long COVID or post-COVID conditions. Updated June 17, 2022. https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html Lopez-Leon S, Wegman-Ostrosky T, Perelman C, et al. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci Rep 2021;11:16144. Sanchez-Ramirez DC, Normand K, Zhaoyun Y, Torres-Castro R. Long-term impact of COVID-19: A systematic review of the literature and meta-analysis. Biomedicines 2021;9:900. |
References
- Saydah SH, Brooks JT, Jackson BR. Surveillance of post-COVID conditions is necessary: Addressing the challenges with multiple approaches. J Gen Intern Med 2022;37:1786-1788.
- Kalish H, Klumpp-Thomas C, Hunsberger S, et al. Undiagnosed SARS-CoV-2 seropositivity during the first 6 months of the COVID-19 pandemic in the United States. Sci Transl Med 2021;13:eabh3826.
- Wanga V, Chevinsky JR, Dimitrov LV, et al. Long-term symptoms among adults tested for SARS-CoV-2 - United States, January 2020-April 2021. MMWR Morb Mortal Wkly Rep 2021;70:1235-1241.
- Jiang DH, Roy DJ, Gu BJ, et al. Postacute sequelae of severe acute respiratory syndrome coronavirus 2 infection: A state-of-the-art review. JACC Basic Transl Sci 2021;6:796-811.
Neurologic Symptoms
How common are neurologic long COVID symptoms, such as brain fog and headache?
The five most common symptoms of long COVID are fatigue (58%), headache (44%), attention-deficit disorder (27%), hair loss (25%), and dyspnea (24%). Various neurologic symptoms of post-acute COVID syndrome (PACS) include headaches, memory deficits, difficulty concentrating, and cognitive impairment (brain fog).1
Post-COVID fatigue represents one of the most persistent and debilitating symptoms following infection. The multiple mechanisms for fatigue post-COVID should be considered in the patient’s differential diagnosis and treatment plan. Mechanisms for fatigue include:2
- inflammation caused by the release of pro-inflammatory cytokines (cytokine storm);
- mitochondrial dysfunction;
- autonomic nervous system abnormalities;
- reduced systemic oxygen extraction;
- poor nutritional status related to loss of taste and smell;
- obesity and physical inactivity;
- muscle wasting (sarcopenia);
- sleep alterations;
- excessive respiratory effort related to respiratory complications;
- depression.
Headache is the most common neurologic symptom. Many patients report headache during and after COVID-19 infection. The characteristics of the headache may resemble migraine or tension-type headache and are treated like the headaches they resemble. There are no symptoms specific for headache related to COVID-19. Headaches can occur in people with a history of prior headaches, but they also can occur in people without a previous headache history.
Neuropsychiatric symptoms also are common after COVID-19 infection, occurring in 30% to 40% of patients.3 Approximately one-third of COVID-19 survivors were diagnosed with generalized anxiety disorders, one-quarter with sleep disorders, 20% with depression, and 12% with post-traumatic stress disorder. The etiology of neuropsychiatric symptoms in COVID-19 patients is complex and multifactorial. Symptoms may be the result of direct effects from infection, including hospitalization and treatment, cerebrovascular disease (including micro-thrombosis), physiological compromise (hypoxia), side effects of medications, or social aspects of having a potentially fatal illness. New preliminary reports suggest that a biomarker, the SARS-CoV-2 spike protein, may further categorize this disorder, since it has been found in blood samples from more than half of the patients studied at Brigham and Women’s Hospital in Boston. Identifying such biomarkers would assist the work to further decipher post-acute sequelae of COVID-19.
Adults have an increased risk of being diagnosed with a new psychiatric disorder after COVID-19 infection. The most common psychiatric conditions presented were anxiety disorders, insomnia, and dementia. Sleep disturbances also may contribute to the presentation of psychiatric disorders.4
References
- Groff D, Sun A, Ssentongo AE, et al. Short-term and long-term rates of postacute sequelae of SARS-CoV-2 Infection: A systematic review. JAMA Netw Open 2021;4:e2128568.
- Azzolino D, Cesari M. Fatigue in the COVID-19 pandemic. Lancet Healthy Longev 2022;3:e128-e129.
- Nalbandian A, Sehgal K, Gupta A, et al. Post-acute COVID-19 syndrome. Nat Med 2021;27:601-615.
- Lopez-Leon S, Wegman-Ostrosky T, Perelman C, et al. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci Rep 2021;11:16144.
Pulmonary Concerns
What are the common pulmonary concerns associated with long COVID?
The most common respiratory symptoms reported between 60 and 100 days after hospital discharge are dyspnea, in as many as two-thirds of patients, and cough, in approximately 16% to 18% of patients. At one year, the prevalence of both dyspnea (in 23% to 25%) and cough (in 2% to 13%) decreased, respectively.1-5 Female gender, number of comorbidities, number of symptoms at the time of admission, and length of admission have been identified as individual risk factors correlating with dyspnea seven months after discharge.6 Higher BMI is associated with persistent dyspnea at one year.7 Several recent studies investigated the effect of pulmonary rehabilitation programs (PRP) on dyspnea progression in these patients. Although more study is needed, findings appear to suggest improvement in respiratory function, exercise capacity, and dyspnea are possible with PRP.8
Pulmonary function tests (PFT) generally are normal in patients following mild or moderate COVID-19 infection.9 However, in patients with severe infection, impaired diffusing capacity of the lungs for carbon monoxide < 80% is the most common pulmonary function test abnormality, seen in almost half of the patients at three to four months, decreasing to 21% at one year. Risk factors for reduced diffusion capacity and poor recovery include female gender, preexisting lung disease, smoking, and ICU admission.7,10 Restrictive ventilatory defects with decreased total lung capacity (TLC) also are directly associated with disease severity.11 Reduced six-minute walk distance, also referred to as 6-MWD, assessed as
< 80% of predicted, was present in 20% of patients at three months, with significant improvement demonstrated at one year with prevalence of 7%.7,12
Radiographic abnormalities, including ground-glass opacities and fibrosis, are present in about one-third of patients six months after severe COVID-19 infection. This finding is directly correlated with age, length of admission, acute respiratory distress syndrome, mechanical ventilation, and the presence of cough.9,13,14 At one year, many patients show improvement, with only 10% having non-progressive fibrotic changes on computed tomography (CT) scan.7
Current recommendations are to perform a baseline assessment within three months after hospitalization by using PFTs, 6-MWDs, and chest radiography, followed serially at six months to one year. Further evaluation with high-resolution CT chest or echocardiogram may be needed for persistent symptoms or severe disease.15,16 There is growing evidence that pulmonary rehabilitation can improve 6-MWD and decrease fatigue and dyspnea, independent of disease severity.17,18 A course of corticosteroids also may be beneficial in a subset of patients with post-COVID-19 interstitial lung disease with organizing pneumonia.19,20 Lung transplantation is reserved for patients with significant debility or progressive disease failing medical therapy.15 Clinical trials currently are underway investigating the role of antifibrotic agents, such as pirfenidone or nintedanib, in the prevention of pulmonary fibrosis and other respiratory complications in COVID-19 survivors.21
References
- Chopra V, Flanders SA, O’Malley M, et al. Sixty-day outcomes among patients hospitalized with COVID-19. Ann Intern Med 2021;174:576-578.
- Garrigues E, Janvier P, Kherabi Y, et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J Infect 2020;81:e4-e6.
- Carfì A, Bernabei R, Landi F; Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent symptoms in patients after acute COVID-19. JAMA 2020;324:603-605.
- Millet C, Narvaneni S, Chaudhry S, et al. The long haul: A follow-up study of patients diagnosed with COVID-19 one year ago at an urban medical center in New Jersey. Chest 2021;160:A566-A567.
- Fernández-de-Las-Peñas C, Guijarro C, Plaza-Canteli S, et al. Prevalence of post-COVID-19 cough one year after SARS-CoV-2 infection: A multicenter study. Lung 2021;199:249-253.
- Fernández-de-Las-Peñas C, Palacios-Ceña D, Gómez-Mayordomo V, et al. Fatigue and dyspnoea as main persistent post-COVID-19 symptoms in previously hospitalized patients: Related functional limitations and disability. Respiration 2022;101:132-141.
- Lorent N, Vande Weygaerde Y, Claeys E, et al. Prospective longitudinal evaluation of hospitalised COVID-19 survivors 3 and 12 months after discharge. ERJ Open Res 2022;8:00004-2022.
- Esque AM, Arias PC, Lostes SS, et al. Impact of pulmonary rehabilitation on sequelae produced in critically ill patients by COVID-19. Eur Respir J 2021;58:PA2263
- Guler SA, Ebner L, Aubry-Beigelman C, et al. Pulmonary function and radiological features 4 months after COVID-19: First results from the national prospective observational Swiss COVID-19 lung study. Eur Respir J 2021 Apr 29;57:2003690.
- Bellan M, Soddu D, Balbo PE, et al. Respiratory and psychophysical sequelae among patients with COVID-19 four months after hospital discharge. JAMA Netw Open 2021;4:e2036142.
- Mo X, Jian W, Su Z, et al. Abnormal pulmonary function in COVID-19 patients at time of hospital discharge. Eur Respir J 2020;55:2001217.
- Wu X, Liu X, Zhou Y, et al. 3-month, 6-month, 9-month, and 12-month respiratory outcomes in patients following COVID-19-related hospitalisation: A prospective study. Lancet Respir Med 2021;9:747-754.
- Han X, Fan Y, Alwalid O, et al. Six-month follow-up chest CT findings after severe COVID-19 pneumonia. Radiology 2021;299:E177-E186.
- Mumoli N, Bonaventura A, Colombo A, et al. Lung function and symptoms in post-COVID-19 patients: A single-center experience. Mayo Clin Proc Innov Qual Outcomes 2021;5:907-915.
- King CS, Mannem H, Kukreja J, et al. Lung transplantation for patients with COVID-19. Chest 2022;161:169-178.
- Bai C, Chotirmall SH, Rello J, et al. Updated guidance on the management of COVID-19: From an American Thoracic Society/European Respiratory Society coordinated International Task Force (29 July 2020). Eur Respir Rev 2020;29:200287.
- Büsching G, Zhang Z, Schmid JP, et al. Effectiveness of pulmonary rehabilitation in severe and critically ill COVID-19 patients: A controlled study. Int J Environ Res Public Health 2021;18:8956.
- Gloeckl R, Leitl D, Jarosch I, et al. Benefits of pulmonary rehabilitation in COVID-19: A prospective observational cohort study. ERJ Open Res 2021;7:00108-2021.
- Myall KJ, Mukherjee B, Castanheira AM, et al. Persistent post-COVID-19 interstitial lung disease. An observational study of corticosteroid treatment. Ann Am Thorac Soc 2021;18:799-806.
- Vadász I, Husain-Syed F, Dorfmüller P, et al. Severe organising pneumonia following COVID-19. Thorax 2021;76:201-204.
- ClinicalTrials.gov. A study to evaluate the efficacy and safety of pirfenidone with novel coronavirus infection. https://clinicaltrials.gov/ct2/show/NCT04282902
Cardiac Complications
What are some of the cardiac complications of post-acute sequelae of COVID-19?
Cardiovascular complications in acute and post-acute sequelae of COVID-19 (PASC) have been well documented in the literature. The COVID-19 outbreak affected 892 ongoing clinical trials in cardiology.1 Since then, more than 100 trials have been registered to investigate cardiovascular complications.2 The term PASC-CVD (post-acute sequelae of COVID-19 cardiovascular disease) describes the collection of cardiovascular diseases that emerge or persist four or more weeks after an acute COVID-19 infection.3 PASC may affect 10% to 30% of COVID-19 patients.4
As the prevalence of PASC increases, clinicians will need to be familiar with:
- the spectrum of cardiovascular complications;
- the pathophysiology of the complications;
- current practice guidelines for the evolving management of these patients.
A study comparing 153,760 COVID-19 patients with contemporary and historical controls evaluated the risk and the 12-month burden of incident cardiovascular disease. Notably, PASC-CVD was observed in low-risk COVID-19 patients who had not been hospitalized and had no past medical history of CVD. The risk and burden of PASC-CVD increased as the severity of the acute COVID-19 infection increased and remained significant, after controlling for demographic and comorbidity variables.5 Cardiovascular manifestations of PASC were diverse and spanned the spectrum of cardiovascular pathology, including thromboembolic disease, inflammatory myocarditis/pericarditis, dysrhythmias, ischemic heart disease, and cerebrovascular disorders.5
The pathophysiological mechanisms underlying PASC-CVD are poorly characterized and multifactorial, potentially accounting for the diversity of its manifestations.6 Direct cardiomyocyte damage from viral invasion, fibrosis, and cardiac remodeling from cytokine upregulation, micro-angiopathy from complement activation, and autoimmunity from hyperactive immune response all have been implicated.7-12 Trials on pharmacotherapies targeting these pathways have been small, have been underpowered, or have had neutral outcomes.2
The American College of Cardiology (ACC) released an expert consensus document regarding the evaluation and management of PASC-CVD, noting that these best practices continue to evolve.3 In symptomatic patients, the ACC recommended advanced testing, guided by clinical circumstance, including laboratory testing, electrocardiograms, echocardiography, and ambulatory rhythm monitoring. It encouraged early cardiology involvement, symptom-guided management, and an emphasis on graded exercise regimens.3
Given the rising incidence of PASC-CVD even in low-risk patients with mild disease, primary COVID-19 prevention should be prioritized. Familiarity with the diagnosis and evolving management of these chronic complications will be a necessity for primary care clinicians.
References
- Selvaraj S, Greene SJ, Khatana SAM, et al. The landscape of cardiovascular clinical trials in the United States initiated before and during COVID-19. J Am Heart Assoc 2020;9:e018274.
- Satterfield BA, Bhatt DL, Gersh BJ. Cardiac involvement in the long-term implications of COVID-19. Nat Rev Cardiol 2021;19:332-341.
- Writing Committee; Gluckman TJ, Bhave NM, Allen LA, et al. 2022 ACC Expert Consensus Decision Pathway on Cardiovascular Sequelae of COVID-19 in Adults: Myocarditis and Other Myocardial Involvement, Post-Acute Sequelae of SARS- CoV-2 Infection, and Return to Play: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol 2022;79:1717-1756.
- Logue JK, Franko NM, McCulloch DJ, et al. Sequelae in adults at 6 months after COVID-19 infection. JAMA Netw Open 2021;4:e210830.
- Xie Y, Xu E, Bowe B, Al-Aly Z. Long-term cardiovascular outcomes of COVID-19. Nat Med 2022;28:583-590.
- Nalbandian A, Sehgal K, Gupta A, et al. Post-acute COVID-19 syndrome. Nat Med 2021;27:601-615.
- Farshidfar F, Koleini N, Ardehali H. Cardiovascular complications of COVID-19. JCI Insight 2021;6:e148980.
- Nishiga M, Wang DW, Han Y, et al. COVID-19 and cardiovascular disease: From basic mechanisms to clinical perspectives. Nat Rev Cardiol 2020;17:543-558.
- Chung MK, Zidar DA, Bristow MR, et al. COVID-19 and cardiovascular disease: From bench to bedside. Circ Res 2021;128:1214-1236.
- Delorey TM, Ziegler CGK, Heimberg G, et al. COVID-19 tissue atlases reveal SARS-CoV-2 pathology and cellular targets. Nature 2021;595:107-113.
- Song W-C, FitzGerald GA. COVID-19, microangiopathy, hemostatic activation, and complement. J Clin Invest 2020;130:3950-3953.
- Varga Z, Flammer AJ, Steiger P, et al. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020;395:1417-1418.
Gastrointestinal Issues and COVID-19
What are the gastrointestinal issues with COVID-19?
Gastrointestinal complications from COVID-19 can occur during acute infection, continue after resolution of the infection (long COVID), or develop in the weeks or months after infection. Up to one-third of COVID-19 patients present with gastrointestinal complaints, such as nausea, vomiting, or diarrhea.1
Patients with severe COVID-19 are at high risk for developing gastrointestinal dysfunction, including acute liver injury with elevated transaminases, acute cholecystitis, acute pancreatitis, ileus and feeding intolerance, acute colonic pseudo-obstruction, and mesenteric ischemia. Mesenteric ischemia is the most serious gastrointestinal complication reported in critically ill COVID-19 patients and should be considered in a hospitalized patient complaining of severe abdominal pain.1
In about one-half of COVID-19 patients, SARS-CoV-2 RNA is shed in the feces in the week after diagnosis and, in some patients, can continue to shed for many months. The presence of fecal SARS-CoV-2 RNA is associated with gastrointestinal symptoms, suggesting that gastrointestinal tissues are directly infected or serve as a viral reservoir.2,3
Long COVID gastrointestinal symptoms include decreased appetite, nausea, weight loss, abdominal pain, heartburn, dysphagia, diarrhea or constipation, and irritable bowel syndrome.4 A personalized nutritional risk assessment should be completed in patients with sustained decreased appetite, particularly in the elderly and the immunocompromised. The use of antimotility agents to treat diarrhea should be avoided, since it may impair viral clearance.5
References
- The Coronavirus Visualization Team. COVID long-haulers: Gastrointestinal system. Harvard University. https://scholar.harvard.edu/cvt/covid-long-haulers-gastrointestinal-system%C2%A0
- Nalbandian A, Sehgal K, Gupta A, et al. Post-acute COVID-19 syndrome. Nature Med 2021;27:601-615.
- Blackett JW, Wainberg M, Elkind MSV, Freedberg DE. Potential long coronavirus disease 2019 gastrointestinal symptoms 6 months after coronavirus infection are associated with mental health symptoms. Gastroenterology 2022;162:648-650.
- Meringer H, Mehandru S. Gastro-intestinal post-acute COVID-19 syndrome. Nat Rev Gastroenterol Hepatol 2022;19:345-346.
- Kow CS, Hasan SS. The use of antimotility drugs in COVID-19 associated diarrhea. J Infect 2021;82:e19.
Diabetes and COVID-19
How does diabetes fit into the COVID-19 picture?
In addition to blood clots, pneumonia, and other complications associated with a SARS-CoV-2 infection, recent studies have identified yet another worrisome association: new-onset diabetes.
Earlier findings had established the connection between diabetes patients and an increased risk of developing a COVID-19 infection, as well as a worsening of diabetes symptoms from the presence of a COVID-19 infection.1 More recent studies have suggested that non-diabetic individuals with COVID-19 may be at risk of receiving a new diabetes diagnosis shortly following infection.
A recent report in Morbidity and Mortality Weekly Report from the CDC demonstrates that persons younger than 18 years of age with COVID-19 were more likely to receive a new diabetes diagnosis greater than 30 days after infection than were those without COVID-19, based on health claims data. The diabetes risk for COVID-19 patients younger than 18 years of age was dramatically higher (31% to 166%) than for those never infected with the virus.2
Diabetes prevalence appears to rise as severity in COVID-19 disease increases, from 6.4% in non-hospitalized patients to 32.4% in intensive care unit patients.3 A study by Montefusco et al found that one-third of newly hyperglycemic individuals remained hyperglycemic for at least six months following their recovery from COVID-19.4 Whether the hyperglycemia causes the poor COVID-19 infection outcomes or if it reflects poor outcomes remains unclear.
Researchers have found that the SARS-CoV-2 virus can affect the pancreas in one of three ways.5-8 First, it may cause direct damage to pancreatic insulin-producing beta cells, inhibiting them from producing enough insulin to control blood sugar levels. Second, the viral replication within the pancreas can damage the cells that directly surround the beta cells, which are needed for appropriate insulin release. Finally, the virus may reprogram any surviving cells, causing them to malfunction and disrupt proper blood sugar regulation.
Additional work has shown another potential cause for newly acquired diabetes in COVID-19-infected patients. According to Zickler et al, SARS-CoV-2 can replicate in human adipose tissue.9 It may cause the adipocytes to send incorrect messages to other cells.
A study by Reiterer et al discovered that COVID-19-infected patients had low levels of adiponectin, a hormone produced by adipocytes that modulates glucose regulation and fatty acid oxidation.10 Therefore, new findings are suggesting that the hyperglycemia in COVID-19 patients is the result of insulin resistance from improper fat hormone levels rather than an inability of pancreatic cells to produce insulin.
Evidence suggests that insulin and dipeptidyl peptidase 4 inhibitors can be used safely in patients with diabetes mellitus and COVID-19. Metformin and sodium-glucose cotransporter 2 inhibitors might need to be withdrawn in patients at high risk of severe disease. Many pharmacological agents currently under investigation for the treatment of COVID-19 can affect glucose metabolism, especially in diabetes patients, requiring frequent blood glucose monitoring and adjustment of medications. Thiazolidinediones, such as pioglitazone, can mediate protective effects on the cardiovascular system. However, the use of this drug class remains unsupported in COVID-19 patients, since heart failure can be aggravated.11
References
- Guo W, Li M, Dong Y, et al. Diabetes is a risk factor for the progression and prognosis of COVID-19. Diabetes Metab Res Rev 2020;36:e3319.
- Barrett CE, Koyama AK, Alvarez P, et al. Risk for newly diagnosed diabetes > 30 days after SARS-CoV-2 infection among persons aged < 18 years — United States, March 1, 2020-June 28, 2021. MMWR Morb Mortal Wkly Rep 2022;71:59-65.
- CDC COVID-19 Response Team. Preliminary estimates of the prevalence of selected underlying health conditions among patients with coronavirus disease 2019 – United States, February 12-March 28, 2020. MMWR Morb Mortal Wkly Rep 2020;69:382-386.
- Montefusco L, Ben Nasr M, D’Addio F, et al. Acute and long-term disruption of glycometabolic control after SARS-CoV-2 infection. Nat Metab 2021;3:774-785.
- Tang X, Uhl S, Zhang T, et al. SARS-CoV-2 infection induces beta cell transdifferentiation. Cell Metab 2021;33:1577-1591.e7.
- Wu CT, Lidsky PV, Xiao Y, et al. SARS-CoV-2 infects human pancreatic β cells and elicits β cell impairment. Cell Metab 2021;33:1565-1576.e5.
- Yang L, Han Y, Nilsson-Payant BE, et al. A human pluripotent stem cell-based platform to study SARS-CoV-2 tropism and model virus infection in human cells and organoids. Cell Stem Cell 2020;27:125-136.e7.
- Müller JA, Groß R, Conzelmann C, et al. SARS-CoV-2 infects and replicates in cells of the human endocrine and exocrine pancreas. Nat Metab 2021;3:149-165.
- Zickler M, Stanelle-Bertram S, Ehret S, et al. Replication of SARS-CoV-2 in adipose tissue determines organ and systemic lipid metabolism in hamsters and humans. Cell Metab 2022;34:1-2.
- Reiterer M, Rajan M, Gómez-Banoy N, et al. Hyperglycemia in acute COVID-19 is characterized by insulin resistance and adipose tissue infectivity by SARS-CoV-2. Cell Metab 2021;33:
2174-2188.e5. - Lim S, Bae JH, Kwon H-S, Nauck MA. COVID-19 and diabetes mellitus: From pathophysiology to clinical management. Nat Rev Endocrinol 2021;17:11-30.
Conclusion: The End of the Pandemic?
For more than two years, people around the world have asked this question:
When will COVID-19 end?
The pandemic has claimed more than 6 million lives worldwide, with more than 1 million documented in the United States.1 COVID-19 has brought increased stress, anxiety, frustration, and fear. Although people remain optimistic that things are improving, this pandemic is not yet over.
The American Psychological Association’s Stress in America survey sheds light on the effect the pandemic has had on the American population.2 More than 60% of people report their lives as permanently changed. The effects of the pandemic on individuals have included increased unhealthy habits, decreased sleep, and worsening mental health.2 Hospitals and their healthcare systems have reorganized patient care, introducing more telehealth options along with employee resource support. It has created a positive shift toward addressing mental health, including patient-, caregiver-, and child-focused needs, as well as rewarding healthcare professional heroes and providing programming to prevent healthcare professional burnout.
A recent survey from Axios/Ipsos shows that Americans no longer view the pandemic as a serious crisis.3 More people view the pandemic as “not a problem at all” vs. a “serious crisis.” Nearly 75% of people see the COVID-19 pandemic as a manageable problem moving forward.3 Data show how the American population has endured and is recovering from the adverse effects of this pandemic. Some Americans maintain resiliency and optimism; yet, education helping to limit misinformation remains a necessity in persevering through the pandemic’s effects.
Omicron variants of the coronavirus SARS-CoV-2 pose a daunting public health emergency. The COVID-19 virus is constantly changing and accumulating mutations in its genetic code over time, resulting in new variants with high transmissibility.4 As social distancing restrictions lessen and Americans reduce mask use, variants able to evade immunity continue to emerge. With vaccination rates still less than optimum, vaccine refusal has continued to be a barrier to bringing this virus under control.5 Second-generation vaccines, now deemed necessary, will be available soon, hopefully leading to less frequent calls for booster doses.
The pandemic continues to contribute to ever-present healthcare issues, such as inequality in access to safe, quality care.6 Patients continue to endure stressors caused by COVID-19, promoting the need for current and relevant education. Healthcare providers can use the educational tools provided in this article as a framework to promote the health and well-being of their patients.
References
- World Health Organization. United States of America situation. https://covid19.who.int/region/amro/country/us
- American Psychological Association. Stress in America: Money, inflation, war pile on to nation stuck in COVID-19 survival mode. https://www.apa.org/news/press/releases/stress/2022/march-2022-survival-mode?utm_source=twitter&utm_medium=social&utm_campaign=apa-stress&utm_content=sia-mar2022-parents#parents
- Jackson C, Newall M, Diamond J, et al. Americans divided over when to return “normal.” Ipsos. Published June 14, 2022. https://www.ipsos.com/en-us/news-polls/axios-ipsos-coronavirus-index
- Centers for Disease Control and Prevention. Variant proportions. http://covid.cdc.gov/covid-data-tracker/#variant-proportions
- Haque A, Pant AB. Mitigating Covid-19 in the face of emerging virus variants, breakthrough infections and vaccine hesitancy. J Autoimmun 2022;127:102792.
- Chowkwanyun M, Reed AL Jr. Racial health disparities and Covid-19—caution and context. N Engl J Med 2020;383:201-203
The members of the WSU-BSOM COVID-19 Education Task Force are: Maaz Arif, MD; Steven Borchers, MS4, MD Candidate; Leah Burke, MS4, MD Candidate; Jacob Butman, BS, MS4, MD Candidate; Lisa Aron Carter, MD; Katie L. Fletcher, BS, MS4, MD Candidate; We’am Hussain, MD; Ariel L. Lanier, MS4, MD Candidate; Deanne Darlene Locker, MS4, MD Candidate; Noah Parker, BA, MS2, MD Candidate; Melanie Alexandra Sich, MS4, MD Candidate; Miriam Malak Soliman, MS3, MD Candidate; Muhammad A. Soofi, MD; Tiffani R. Spaulding, MPH, MS3, MD Candidate; Daniel Von Der Vellen, MS3, MD Candidate; and Joy I. Wang, MD.