A Slow But Regular Rhythm Pattern
By Ken Grauer, MD
Professor Emeritus in Family Medicine, College of Medicine, University of Florida
The tracing below was obtained from an older woman with a slow pulse. How should one interpret the ECG?
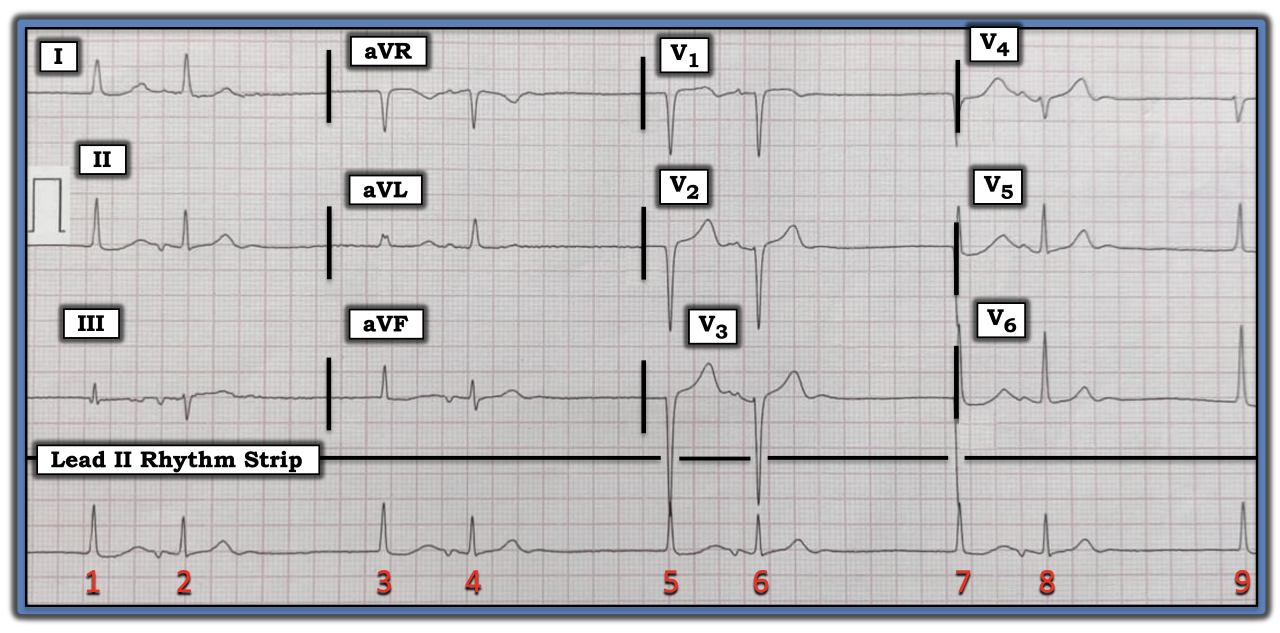
This patient was hemodynamically stable in association with this slow rhythm. My attention was captured by the “regular irregularity” of this rhythm — in the form of a “bigeminal” rhythm (i.e., with repetitive groups of two beats that are separated by short pauses of similar duration). Note the lack of sinus P waves (i.e., no upright P waves are seen anywhere on this long lead II rhythm strip). Instead, all P waves on this tracing are negative (i.e., non-sinus) and seen after the initial QRS complex in each group. The QRS complex is narrow for all nine beats. This confirms all QRS complexes are supraventricular. That said, the two QRS complexes in each two-beat group look at least slightly different in many of the 12 leads.
The rhythm represents a slow, supraventricular bigeminal rhythm, with repetitive two-beat groups. No P wave precedes the first narrow QRS complex in each group (i.e., there is no P wave in front of beats 1, 3, 5, 7, or 9). The R-R interval preceding each beat is between seven to eight large boxes in duration (corresponding to a ventricular rate of close to 40 beats/minute). Therefore, the initial beat in each group is a junctional “escape” beat at an appropriate junctional escape rate.
The fact the P waves that follow beats 1, 3, 5, and 7 all are negative, with a relatively long coupling interval (distance from the preceding junctional QRS complex) suggests these P waves are conducted retrograde (backward) to the atria. Also, this retrograde conduction then can “turn around” and conduct downward to “capture” the ventricles.
The rhythm is known as “escape-capture” bigeminy. It does not necessarily imply any AV block. Instead, the primary problem likely is to be marked sinus bradycardia at a rate that is slower than the noted junctional “escape” rate. It may be that stopping a rate-slowing medication (e.g., a beta-blocker or the calcium channel blocker verapamil) will be all that is needed to resolve the problem. Alternatively, if this elderly patient is not on any rate-slowing medication, and there is no other “fixable” cause (such as recent ischemia/infarction, hypothyroidism, or sleep apnea), then it becomes likely this rhythm is a manifestation of sick sinus syndrome, for which the patient might need a permanent pacemaker.
For further discussion of and more information about this case, please visit: https://bit.ly/3PSmtgz.
The tracing was obtained from an older woman with a slow pulse. How should one interpret the ECG?
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.