Why All the P Waves?
ECG Review
Why All the P Waves?
By Ken Grauer, MD, Professor Emeritus in Family Medicine, College of Medicine, University of Florida. Dr. Grauer is the sole proprietor of KG-EKG Press, and publisher of an ECG pocket brain book.
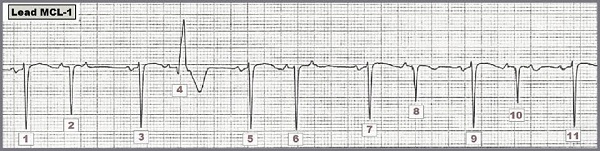
Figure Right-sided MCL-1 monitoring lead rhythm strip. Can you explain the irregularity?
Scenario: Interpret the lead MCL-1 rhythm strip shown above. Can you explain the irregularity?
Interpretation: The easiest way to approach interpretation of challenging arrhythmias is to start with what is known. Save more difficult parts of the tracing until later. We always look first to see if there is an underlying rhythm. The underlying rhythm in the Figure is sinus, as determined by beats #1, #3, #5, #7, #9, and #11. Each of these beats is preceded by a similar-morphology biphasic P wave with fixed PR interval. All QRS complexes except for beat #4 are narrow. Note the interesting bigeminal periodicity of the rhythm with alternating short-long cycles. Every other QRS complex in this tracing occurs early. Every other QRS complex is a premature atrial contraction (PAC).
The rhythm in the Figure is, therefore, sinus with multiple PACs. We highlight a number of additional interesting points about this rhythm: 1) P wave morphology of each PAC is slightly different in being primarily positive compared to the biphasic P waves of each sinus beat. This is as it should be since PACs by definition originate from a different site in the atria than the sinus node. 2) Not all PACs are conducted. Note that no QRS complex follows the PACs that occur just after beats #2, #6, and #10. These PACs are "blocked" (nonconducted) because they arise so early in the cycle as to occur during the absolute refractory period when conduction to the ventricles from an impulse arriving early at the AV node is not possible. 3) The widened QRS complex (beat #4) is not a premature ventricular contraction. Instead, it too is a PAC conducted with aberration. Note that beat #4 is also preceded by a "telltale" premature P wave which confirms that this beat is an aberrantly conducted PAC. 4) In fact, beats #2, #4, #8 and #10 are all aberrantly conducted PACs! Normally, QRS morphology of PACs will be virtually identical to QRS morphology of sinus beats. PACs merely arrive earlier than anticipated at the AV node but once there, they typically conduct to the ventricles in normal fashion. It is only when PACs arrive especially early (or when the relative refractory period is for some reason prolonged) that PACs may manifest aberrant conduction. 5) Beats #2, #4, #8, and #10 are all PACs that manifest different degrees of aberrancy. Of these beats, it is beat #4 that manifests the greatest degree of aberrant conduction (in the form of a complete right bundle branch block pattern). This makes sense because the coupling interval of the PAC preceding beat #4 (distance between this P wave and beat #3) is shorter than the coupling interval for the other PACs. The P wave preceding beat #4 therefore arrives earlier at the AV node at a time when it is more likely to encounter the conduction system in a relatively refractory state. In contrast, the coupling intervals of the P waves following beats #2, #6, and #10 are even shorter. Physiologically, the P waves following beats #2, #6 and #10 are presumably occurring during the absolute refractory period, which is why these PACs are "blocked." In summary, our interpretation of this lead MCL-1 rhythm strip is that it shows underlying sinus rhythm with multiple PACs that are either blocked or conducted with varying degrees of aberration.
Scenario: Interpret the lead MCL-1 rhythm strip shown above. Can you explain the irregularity?Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.