ECG Review: Early Repolarization or Anterior STEMI?
ECG Review: Early Repolarization or Anterior STEMI?
By Ken Grauer, MD, Professor Emeritus in Family Medicine, College of Medicine, University of Florida. Dr. Grauer is the sole proprietor of KG-EKG Press, and publisher of an ECG pocket brain book.
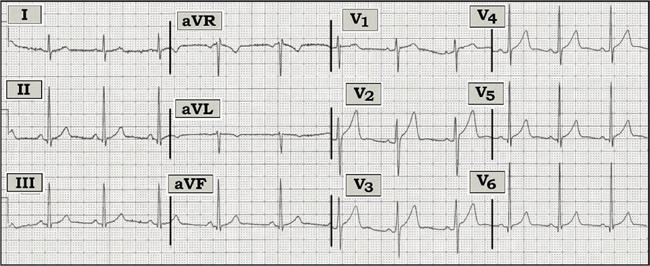
Figure — 12-lead ECG from a 50-year-old man with new-onset chest pain.
Scenario: The 12-lead ECG shown above was obtained from a 50-year-old man with new-onset chest pain. Is this ECG likely to represent a benign early repolarization pattern or the early stage of acute anterior ST elevation myocardial infarction (STEMI)?
Interpretation: The ECG shows sinus arrhythmia with normal intervals and axis, and voltage for left ventricular hypertrophy. There are small q waves in the inferior and lateral precordial leads. R wave progression is normal, with transition occurring between leads V3-to-V4. T waves are peaked. There is some J-point ST segment elevation with upward concavity in virtually all precordial leads, with ST elevation attaining at least 2 mm in lead V2. In addition, there is shallow symmetric T wave inversion in lead aVL.
The significance of the findings identified in the above tracing depends greatly on the clinical setting. Overall, this ECG has the appearance of early repolarization pattern (ERP) because:
1) ST segments manifest an upward concavity (“smiley” configuration) rather than a coved (downward convexity or “frowny” pattern) that would be suggestive of acute injury.
2) ST segment elevation is not marked in amount.
3) The q waves that are seen are small and narrow, which is consistent with normal septal q waves.
4) Other than isolated shallow T wave inversion in lead aVL (which may be a normal finding, especially given the predominantly negative QRS complex in this lead), there are no reciprocal ST-T wave changes.
Despite the above factors in favor of ERP, one cannot rule out the possibility of early anterior STEMI on the basis of this single ECG because there is ST segment elevation, and the patient is a 50-year-old man with new-onset chest pain. Early changes of anterior STEMI may be subtle, and ST segment elevation may (at least initially) manifest an upward concavity. Clinical follow-up is urgently needed. Search for a prior tracing on this patient, repeating the ECG in short order (to see if there is evolution), serial troponins, and close observation over ensuing hours should be revealing as to what (if anything) is occurring.
For more information on ERP and how to distinguish ERP from anterior STEMI, please visit: https://www.kg-ekgpress.com/ecg_-_early_repolarization/.
The 12-lead ECG shown above was obtained from a 50-year-old man with new-onset chest pain. Is this ECG likely to represent a benign early repolarization pattern or the early stage of acute anterior ST elevation myocardial infarction (STEMI)?Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.