ECG Review: Atypical Chest Pain and Early Repolarization?
Atypical Chest Pain and Early Repolarization?
By Ken Grauer, MD
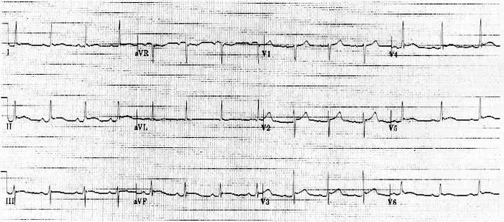
Figure. 12-lead ECG recorded from a 23-year-old man with atypical chest pain.
Clinical Scenario: The ECG in the Figure was obtained from a 23-year-old male who presented with a several day history of atypical chest pain. His ECG was interpreted as consistent with an early repolarization variant. Should anything else be considered in the differential?
Interpretation: The ECG in the Figure shows a normal sinus rhythm at a rate of about 85 beats/minute. All intervals are normal. The mean QRS axis is about +30°. There is no chamber enlargement. The most remarkable finding on this tracing is the presence and nature of ST segment elevation. Although subtle in some leads, at least some amount of ST segment elevation is seen in virtually all leads except leads III, aVR, and V1. Although the patient's age and the presence of J point notching in several leads are certainly consistent with a normal variant early repolarization pattern, the diffuse nature of the ST segment elevation seen here, as well as its shape (coved in several leads) should make one suspect that something else may be going on.
Myocardial ischemia or infarction is highly unlikely in a 23 year-old (assuming there is no history of cocaine ingestion), especially in the absence of significant Q waves and reciprocal ST segment depression. Instead the presence of diffuse ST segment elevation without reciprocal changes in a young adult with atypical chest pain should suggest the possibility of acute pericarditis. Eliciting a history of a recent viral illness would be supportive, and hearing a pericardial friction rub on physical exam would be virtually diagnostic. This is in fact what this patient had.
The initial stage of acute pericarditis is characterized by diffuse (sometimes J point) ST segment elevation in virtually all leads except III, aVR and V1. As opposed to acute inferior myocardial infarction in which the ECG pattern in lead III is often very similar to that in lead II, with acute pericarditis it is lead I that much more resembles the ECG pattern in lead II (as is the case here). PR segment depression may be a helpful supportive sign of acute pericarditis when present, though it is not seen here. The point to emphasize is that the normal variant pattern of early repolarization should only be thought of as a diagnosis of exclusion after acute infarction or pericarditis have been ruled out.
Dr. Grauer, Professor, Assistant Director, Family Practice Residency Program, University of Florida, is Associate Editor of Internal Medicine Alert.
The ECG in the Figure was obtained from a 23-year-old male who presented with a several day history of atypical chest pain. His ECG was interpreted as consistent with an early repolarization variant. Should anything else be considered in the differential?
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.