By Ken Grauer, MD
Professor Emeritus in Family Medicine, College of Medicine, University of Florida
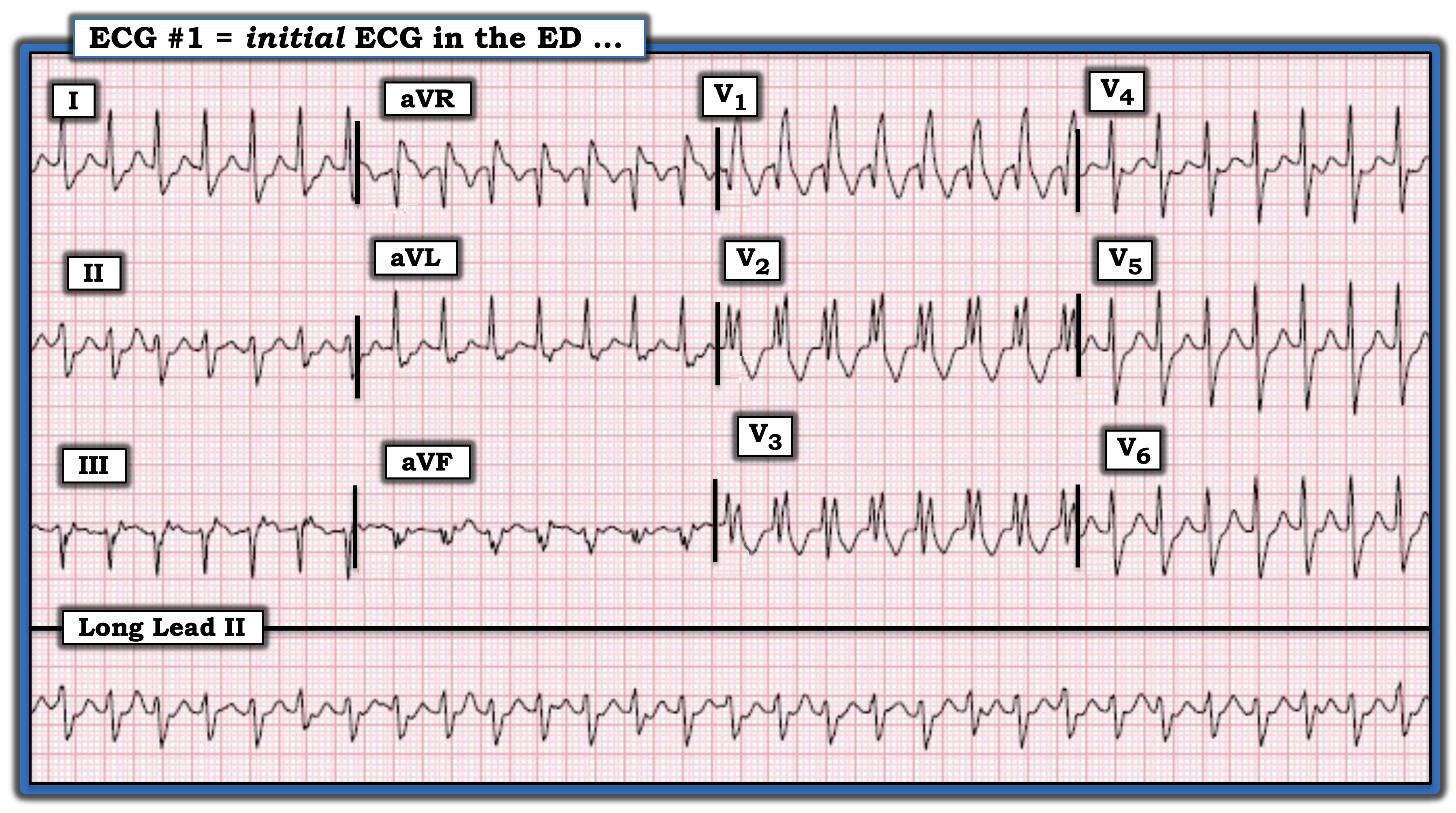
How would one interpret the tachycardia in the ECG below? Is the rhythm ventricular tachycardia (VT) or some form of supraventricular tachycardia (SVT)? How should one proceed?
Notably absent is a brief history, such as age, symptoms, prior episodes, or family heart disease. The highest priority is to immediately assess whether the patient is hemodynamically stable in association with this rhythm. If not, then regardless of the etiology of the tachycardia immediate synchronized cardioversion will be indicated. It turned out the patient was hemodynamically stable at the time this ECG was obtained. By definition, this provided a moment for careful assessment of ECG features.
The rhythm in the figure is a regular wide complex tachycardia (WCT) rhythm at a rate of approximately 180 beats/minute. Sinus P waves are absent because there is no clearly positive upright P wave in lead II. Whether sinus P waves might be hidden within preceding T waves or whether what appears to be a small negative notching shortly after the QRS complex in leads III and aVF might represent retrograde atrial activity is uncertain from this single tracing.
The principal differential diagnosis for the regular WCT rhythm in the figure is between VT vs. some form of SVT with QRS widening from either preexisting bundle branch block or from aberrant conduction. Statistically, most regular WCT rhythms without clear sign of atrial activity will turn out to be VT. That said, QRS morphology strongly suggests a supraventricular etiology for this tracing because of close resemblance to conduction right bundle branch block with left anterior hemiblock (RBBB/LAHB). Characteristic features of RBBB conduction seen in this tracing include a triphasic rSR’ pattern in lead V1, with narrow initial R waves and wide terminal S waves in lateral leads I and V6. The rS morphology seen in each inferior lead is completely consistent with LAHB conduction.
The good news is that since this patient was hemodynamically stable, a trial of medical therapy was warranted. Treatment with a combination of agents successfully converted the rhythm. The follow-up ECG showed sinus rhythm with RBBB, confirming preexisting BBB as the reason for QRS widening during the WCT.
For more information about and further discussion of this case, please click here.

How would one interpret the tachycardia in the ECG? Is the rhythm ventricular tachycardia or some form of supraventricular tachycardia? How should one proceed?
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.