AUTHORS
Jay Bernstein, MD, MPH, MS, FACEP,Assistant Professor, Department of Emergency Medicine, Wright State University, Dayton, OH
Shannon Lyon, MD,Emergency Medicine Resident, Wright State University, Dayton, OH
Rachel Tabbouche,University of Maryland, College Park
PEER REVIEWER
Frank LoVecchio, DO, FACEP,Vice-Chair for Research, Medical Director, Samaritan Regional Poison Control Center, Emergency Medicine Department, Maricopa Medical Center, Phoenix, AZ
Introduction
Multiple sclerosis (MS) is an immune-mediated process causing impairment to the neurons of the optic nerve, brain, and spinal cord. This leads to central nervous system (CNS) demyelination, chronic inflammation, axonal transections, and scarring, manifesting by clinical signs and symptoms and an abnormal magnetic resonance imaging (MRI).
The signs and symptoms of MS can be nonspecific or can mimic other neurologic entities. One study showed that 26.6% of MS diagnoses were missed on presentation to the ED and took up to a year to diagnose in 18.4%.1 Prompt and accurate diagnosis of MS is important for early treatment, since early treatment of MS improves neurologic outcomes.2
There are five subgroups of MS presentations:3
• clinically isolated syndrome (CIS): A self-limited episode that most often is monophasic, lasting at least 24 hours, and most commonly involving the optic nerve or a single area of the brain or the spinal cord;4
• relapsing-remitting MS (RRMS): Progressive MS symptoms with periods of improvement or resolution;
• primary progressive MS (PPMS): A continuous decline in MS from the time of an initial diagnosis of MS without relapses;
• secondary progressive MS (SPMS): This occurs only after the RRMS has been present > 10 years, manifested by a chronic decline with fewer relapses;
• progressive (or primary) relapsing MS (PRMS): A rare variant that is a continual decline in MS from the time of an initial diagnosis of MS.
Although these five subgroups are not always clinically useful, especially in the ED, the utility of citing them is to be aware of the variability of MS presentations.The forms of MS that are associated with acute episodes of disability are due to inflammation vs. degeneration in the progressive subtypes. The rate and degree to which patients develop and remain with disability are highly variable. As symptoms decline over time, age is the only predictor for disease progression.5 Therapies appear to be less beneficial in the older population.6
Epidemiology
Approximately 23 million people are diagnosed with MS worldwide.7 The prevalence of MS in North America is more than 140/100,000, and it is the most common demyelinating disease.8,9 MS is more prevalent in women than men, with a 3:1 ratio, and it is most common among Caucasians.9,10 A majority of MS cases are found in North America and Europe and are less common closer to the equator.11,12 CIS typically occurs between the ages of 20 and 45 years, and 2.5:1 in females to males.13 Optic neuritis CIS progresses to MS with an incidence of 10% to 85%. The incidence of a CIS progressing to MS in the brainstem is 53% to 60%, and to the spinal cord is 41% to 61%.4 RRMS is the most common form of MS, involving 85% of MS cases, and is more prevalent among females.8 RRMS typically presents at 30 years of age, younger than PPMS, and occurs after the onset of RRMS 20% to 50% of the time.3,10,14 PPMS occurs in 10% to 15% of MS patients.15
Etiology
The primary etiology of MS has not been established and it is thought to be multifactorial.16 Risk factors include infections, immunity, genetics, demographics, and environmental influences.17 The Epstein-Barr virus (EBV) is a strong risk factor for MS. Recurrent episodes of RRMS are caused by recurrent EBV infections.18,19 Roseola infantum (human herpesvirus 6) has been associated with an increased risk of MS later in life.17 A previous history of herpes simplex virus and human endogenous retroviruses has been shown to be associated with MS as well.17 Many nonviral environmental exposures have been linked to the development of MS. In adults, onset, relapse, and progression are positively affected by sun exposure and vitamin D levels and negatively by smoking.17 Genetic factors and their relationship to the patient’s environment affect MS risk. Autoimmune diseases share many genetic markers with those of MS, suggesting an overlap between autoimmune diseases and MS.20
Pathophysiology
MS can involve the brain, sphincter, visual, pyramidal, brainstem, cerebellar, or sensory pathways. MS occurs in two stages.21 The first phase is caused by acute inflammatory demyelination, which leads to interruptions within axonal conduction, expressed as flares of symptoms. Six months of persistent demyelination leads to the second phase, which is disability. Disability is a manifestation of a complete loss of axons and mitochondrial dysfunction, which increases the likelihood that these changes are irreversible. This is independent of focal inflammation and can be visualized by MRI. MS signs and symptoms typically present over hours to days and gradually resolve within weeks to months. It can manifest as a lesion of the optic nerve, the brain (including the brainstem, cerebellum, or, less commonly, the cerebrum), and the spinal cord.
Clinical Features
New neurologic complaints consistent with MS develop over hours to days. The typical patient is between 15 and 50 years of age and female.6 The most common presentations of new-onset MS are numbness or weakness of the extremities, followed closely by visual deficits.1
The differential diagnosis for numbness and weakness is broad (see Table 1), but the most specific presentation is an ophthalmologic complaint that presents as unilateral optic neuritis.22 Patients typically will have acute onset of ocular pain with eye movements (92% of cases), usually followed by decreased vision in the same eye, and absence of visible external eye abnormalities. Most often, symptoms will spontaneously improve over several weeks, and the patient typically will have normal vision in six to 12 months. Optic neuritis presents as diminished visual acuity and pain with extraocular movements from the loss of axonal conduction. This pain typically is unilateral and associated with loss of central vision. Flashing lights represent a hyperexcitable symptom of optic neuritis. Optic neuritis can be seen on MRI approximately six months after the onset of symptoms.23 When the brainstem or cerebellum is involved, MS will present most often as bilateral internuclear ophthalmoplegia (INO). MS-induced bilateral INO is caused by inflammation and plaques that cause demyelination present at the site of the medial longitudinal fasciculus (MLF) between the third and sixth cranial nerve (CN) nuclei. This leads to a diminished conjugate gaze when looking to either side. The patient senses it as double vision when looking to the right or left.24 When a lesion of the INO is unilateral, one should consider other diagnoses, such as a stroke. When bilateral INO is present, this is considered to be pathognomonic for MS. 24
Table 1. Differential Diagnosis | |
Vascular | Ischemic stroke, hemorrhagic stroke, transient ischemic attack (TIA), cerebral aneurysm, vertebral/carotid dissection, central venous thrombosis, amaurosis fugax, anemia |
Infectious/ | Severe infection (sepsis), viral encephalitis (including herpes simplex virus [HSV]), bacterial meningitis, Lemierre syndrome, human immunodeficiency virus (HIV), neurosyphilis, systemic lupus erythematosus, polyarteritis nodosa, Lyme disease |
Toxicologic/ | Concussion/traumatic brain injury (TBI), neuropraxia, spinal injury, rhabdomyolysis, ciguatera poisoning, coral snake bite, bark scorpion sting, tick paralysis, botulism, organophosphates, methanol poisoning |
Autoimmune | Guillain-Barré syndrome, myasthenia gravis, Lambert-Eaton syndrome, autoimmune encephalitis |
Metabolic | Hypoglycemia, hypokalemia, hypocalcemia, vitamin B12 deficiency |
Neoplastic | Intracranial tumors, spinal cord tumors, Schwannoma, metastatic lesions |
Congenital | Arnold-Chiari malformation |
Degenerative | Diabetic neuropathy, amyotrophic lateral sclerosis (ALS), Huntington’s disease |
Endocrine | Hypothyroidism, hyperthyroidism |
(In particular, the close mimickers that have a relapsing and remitting course are: neuromyelitis optica, neurosarcoidosis, central nervous system vasculitis, Susac’s syndrome, CADASIL [cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy], systemic lupus erythematosus, Sjögren’s syndrome, antiphospholipid syndrome, Behçet’s disease, CLIPPERS [chronic lymphocytic inflammation with pontine perivascular enhancement responsive to steroids], and Leber’s hereditary optic neuropathy.) | |
Less common presentations involve the cerebrum, which manifest as deficits of language, spatial orientation, memory, and mood.25,26 Spinal cord involvement leads to gait impairment, partial myopathy, Lhermitte sign or phenomenon (electric shocks), paresthesias, erectile dysfunction or urinary urgency or incontinence, and pain of the bladder or bowel.27
Although early recognition and diagnosis of a new onset of MS are important, the emergency physician will encounter and manage those with a known diagnosis of MS more often. The patient with known MS who presents with increasing or additional neurologic symptoms could represent a relapse or a pseudorelapse. Clinically, these can be indistinguishable. The difference is the underlying pathophysiology and treatments.28 An MS relapse, also referred to as a flare, an exacerbation, or an attack, occurs at least one month after a previous MS relapse, and the signs and symptoms will be continuous for at least 12-24 hours or longer. MS relapses are common and unpredictable. They may involve a similar presentation as prior MS episodes or different areas of the nervous system and involve a single symptom 71% of the time.29 An MS relapse affects an additional area in the CNS, and new lesions appear on MRI. New deficits identified that represent a true relapse should be managed by mitigation of new inflammation.
In contrast, a pseudorelapse is when the signs and symptoms result from an exacerbation of an existing area of MS axonal lesions and are intermittent and/or waxing and waning for a duration less than 24 hours. A pseudorelapse will not reveal MRI findings, and it is triggered by a form of stress. The types of stress include fatigue, exertion, infection and/or increased body temperature, exposure to elevated external (air) temperature or humidity, and distended bowel or bladder. Treating a pseudorelapse involves treating the underlying stress. A urinary tract infection (UTI) and an upper respiratory infection (URI) are the most common causes.30 Spinal cord lesions often lead to urinary retention, which increases the risk of a UTI.31 Up to 30% of patients with MS have oropharyngeal dysphagia as well, placing them at risk for aspiration pneumonia and pneumonitis.32 Uhthoff’s phenomenon or Uhthoff’s sign is an exacerbation of MS signs or symptoms from exercise or exposure to heat that occurs in 60% to 80% of patients with MS.33 MS causes a decline in respiration as a result of weak respiratory muscles, bulbar dysfunction, impaired cough, abnormalities of the control of breathing, neurogenic pulmonary edema, and leading to hypercarbia and, less commonly, hypoxia or respiratory arrest.34,35
If the patient has altered mental status or one of the common pain syndromes (chest pain, low back pain, etc.), it is unlikely to represent a pseudorelapse (or a relapse as well), and other non-MS conditions should be considered.36 If neurologic symptoms are hyperacute (seconds to minutes), non-MS conditions, such as hypoglycemia, toxins, seizures, or stroke, need to be considered. Acute onset of symptoms (hours to days) could be caused by meningitis and cerebral venous thrombosis, which is a similar time course onset as MS. A subacute onset (weeks to months) is not consistent with an MS presentation or relapse, and other causes need to be considered, such as malignancies, autoimmune disorders, fungal meningitis, human immunodeficiency virus (HIV)/human T-cell leukemia virus type 1 (HTLV-1), and other metabolic syndromes.36
In addition to the medications listed in Table 2, adjunct medications also can be used. These may include antimuscarinics for bladder dysfunction, antidepressants/anxiolytics, amantadine for fatigue, muscle relaxants, and stimulant medications to aid with cognitive dysfunction.31,37-39
Cognitive Effects
MS patients may have an underlying psychiatric condition that may exacerbate or cloud the clinical picture of an MS flare or pseudorelapse. This includes less emotional expression, depression, or involvement in control issues, including abuse or manipulation by family or friends. Cognitive deficits caused by MS influence the expression of disease or ability to cope. Cognition can affect multitasking, performing activities of daily living (ADLs), concentration, judgment, as well as processing and memory impairment.40,41
When communicating with MS patients in the ED, provide enough time for the patient to verbalize understanding, allow digestible fragments of information, and provide written summaries of results and plans.
MS patients are at a significantly higher risk of developing depression and anxiety.42 This likely is the result of a combination of the inflammatory changes of the brain parenchyma as well as the social impact of a disability.43 Depression is more common in men, which is different from the non-MS population.44 This is exacerbated by the lack of control and uncertainty of the progression of symptoms.45 Depression can reduce compliance with treatments,and many MS medications can exacerbate depression.46 (See Table 2.) There have been multiple proposed screening tools for depression in MS.47 The most practical in the ED is the PHQ-2, since it is simple and efficient. It consists of these two questions.48
1. In the last two weeks, how many days have you had little interest or pleasure in doing things?
2. In the last two weeks, how many days have you felt down, depressed, or hopeless?
The PHQ-2 has an accuracy of 0.84 and a negative predictive value of 0.96.47 This can be a rapid aid in the ED to screen for ongoing depression in MS patients to help guide management, therapy regimens, and disposition decisions.
(Click the tables below to open larger versions in new tabs.)
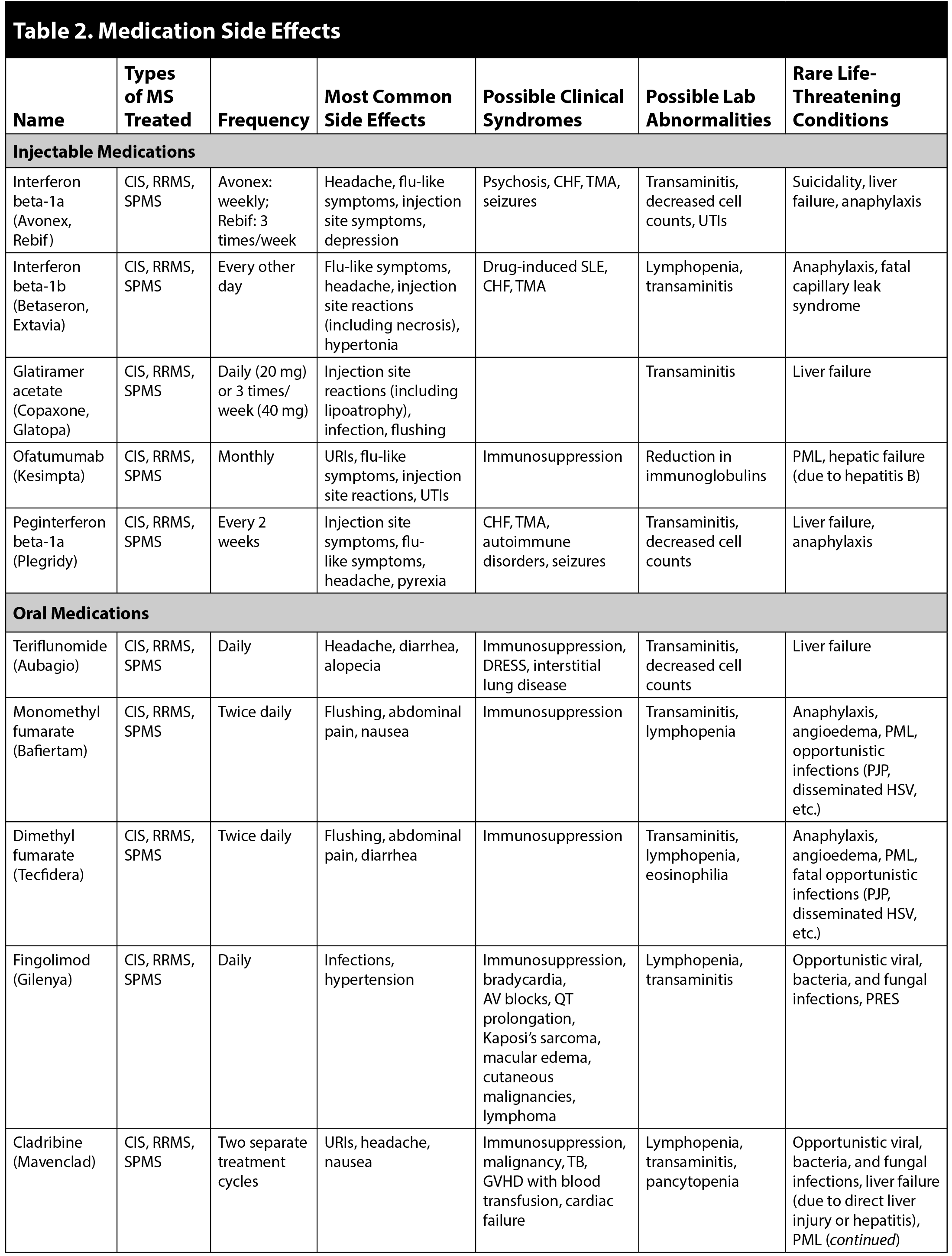
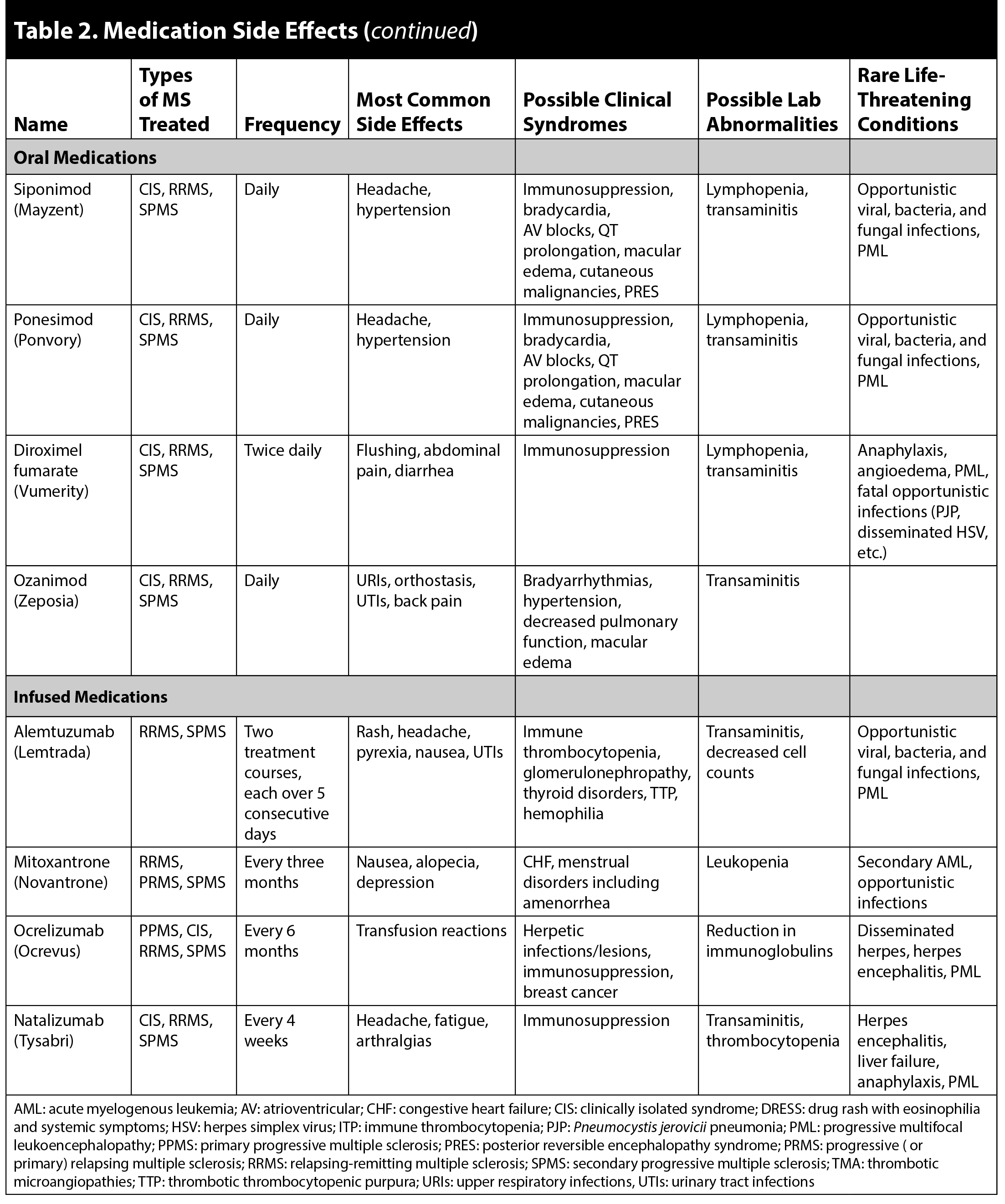
If a patient presents with complaints of new or worsening psychiatric effects, the etiology usually is multifaceted. Changes in mood could be related to physical deficits and their impact on livelihood. Mood changes can be affected by the medications used to treat MS, as noted in Table 2. Medication reconciliation and review of recent changes in medications should be performed in detail.
Behavioral changes can be a result of frontal lobe plaques inherent to the disease process as well, resulting in a lack of normal verbal inhibitions. New psychiatric symptoms may be a sign of a relapse, even in the absence of physical deficits. Dementia is unlikely to be a contributing factor in MS patients, since MS does not increase the risk of dementia or affect intelligence.49
Diagnostic Tools
MS is a clinical diagnosis that requires an array of data and historical factors over time to make. In the history of present illness, elicit the historical neurologic abnormalities that are relevant to the algorithm outlined in the 2017 McDonald criteria.50 (See Table 3.) The 2017 McDonald criteria are not intended to rule out non-MS diagnoses and should not be used by the ED physician to make a final diagnosis.
Table 3. The 2017 McDonald Criteria for Diagnosis of Multiple Sclerosis in Patients with an Attack at Onset | ||
Number of lesions with objective clinical evidence | Additional data needed for a diagnosis of multiple sclerosis | |
≥ 2 clinical attacks | ≥ 2 | None* |
≥ 2 clinical attacks | 1 (as well as clear-cut historical evidence of a previous attack involving a lesion in a distinct anatomical location†) | None* |
≥ 2 clinical attacks | 1 | Dissemination in space demonstrated by an additional clinical attack implicating a different CNS site or by MRI‡ |
1 clinical attack | ≥ 2 | Dissemination in time demonstrated by an additional clinical attack or by MRI§ OR demonstration of CSF-specific oligoclonal bands¶ |
1 clinical attack | 1 | Dissemination in space demonstrated by an additional clinical attack implicating a different CNS site or by MRI‡ AND Dissemination in time demonstrated by an additional clinical attack or by MRI§ OR demonstration of CSF-specific oligoclonal bands¶ |
If the 2017 McDonald Criteria are fulfilled and there is no better explanation for the clinical presentation, the diagnosis is multiple sclerosis. If multiple sclerosis is suspected by virtue of a clinically isolated syndrome but the 2017 McDonald Criteria are not completely met, the diagnosis is possible multiple sclerosis. If another diagnosis arises during the evaluation that better explains the clinical presentation, the diagnosis is not multiple sclerosis. An attack is defined in panel 1. *No additional tests are required to demonstrate dissemination in space and time. However, unless MRI is not possible, brain MRI should be obtained in all patients in whom the diagnosis of multiple sclerosis is being considered. In addition, spinal cord MRI or CSF examination should be considered in patients with insufficient clinical and MRI evidence supporting multiple sclerosis, with a presentation other than a typical clinically isolated syndrome, or with atypical features. If imaging or other tests (eg, CSF) are undertaken and are negative, caution needs to be taken before making a diagnosis of multiple sclerosis, and alternative diagnoses should be considered. †Clinical diagnosis based on objective clinical findings for two attacks is most secure. Reasonable historical evidence for one past attack, in the absence of documented objective neurological findings, can include historical events with symptoms and evolution characteristic for a previous inflammatory demyelinating attack; at least one attack, however, must be supported by objective findings. In the absence of residual objective evidence, caution is needed. ‡The MRI criteria for dissemination in space are described in panel 5. §The MRI criteria for dissemination in time are described in panel 5. ¶The presence of CSF-specific oligoclonal bands does not demonstrate dissemination in time per se but can substitute for the requirement for demonstration of this measure. Reprinted from: Lancet Neurology, vol. 17, issue 2, Thompson AJ, Banwell BL, Barkhof F, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria, page 167, Copyright 2018, with permission from Elsevier. | ||
Alternate diagnoses should be considered as well to ensure a separate phenomenon is not causing the new symptoms (e.g., ischemic stroke, infections, metabolic disturbances). Along with a thorough history and physical exam, obtain a visual field test. A unilateral loss of vision suggests optic neuritis with a scotoma of the central or cecocentral visual field. The monocular vision loss is associated with the presence of relative afferent pupillary defect (RAPD) on exam, otherwise known as a Marcus Gunn pupil. RAPD is elicited by shining a bright flashlight at the unaffected eye in a dark room and swinging the light to the affected eye (with visual loss). In a patient with optic neuritis, this results in a diminished or absent pupillary constriction.
The Lhermitte phenomenon is a relatively unique exam finding of MS that occurs when MS affects the spine. This also is known as the barber chair phenomenon, which is an electric shock-like sensation that occurs in the neck on flexion of the neck. Urinary retention can be seen with a bladder scan. The level of spinal cord involvement determines which symptoms will affect the patient.
MRI is the primary imaging modality that provides diagnostic information by determining a new diagnosis or an exacerbation of MS, or demonstrable progression of chronic MS, and serves to guide treatments.51-53 An MRI is positive in 80% of CIS and is abnormal in nearly 100% of patients with an established diagnosis.54 A spinal MRI is important because almost 50% of patients with a CIS and up to 90% of those with chronic forms of MS have a lesion seen in the spine, usually the cervical spine.55-58 Most commonly, there are foci of abnormalities identified within the white matter, located in the periventricular, infratentorial, or the juxtacortical areas.54
In the ED, obtain a workup that includes a complete blood count, comprehensive metabolic panel, urinalysis, and an electrocardiograph. Check for any signs of neutropenia, lymphopenia, or other signs of immunocompromise. Consider additional testing to evaluate other entities that increase the risk of MS that include a mononucleosis spot test and EBV nuclear antigen immunoglobulin G (IgG) levels.17 Send extra tubes of blood to the lab to add on further possible MS workups, such as myelin-oligodendrocyte glycoprotein (MOG-IgG) antibodies.
When the history, exam, and MRI are not able to provide a clear diagnosis of MS, a lumbar puncture (LP) may be necessary. The cerebrospinal fluid (CSF) in MS demonstrates a normal white blood cell (WBC) count or slight pleocytosis (up to 25 WBCs per cm3), increased protein (under 1 g/L), elevated IgG index, and IgG oligoclonal bands.54 CSF oligoclonal bands are present up to 90% of the time when patients are diagnosed with MS.59
Non-MS-related diagnoses need to be considered. MS is diagnosed incorrectly in up to 10% of cases.60 Common misdiagnoses include fibromyalgia, small vessel cerebrovascular disease, migraine headache, and other functional neurological conditions.60,61
The ED physician should be able to integrate history and clinical exam findings and facilitate further diagnostic studies. Ultimately, a definitive diagnosis of MS should be made by either an MS subspecialist or a neurologist who is familiar with MS diagnostic criteria and treatment.
Management
The most common life-threatening problem is sepsis, typically related to respiratory infections or urinary tract infections.62 Less commonly, complications of medical management listed in Table 1 can occur, including anaphylaxis, immunosuppression leading to fatal opportunistic infections, or hepatic failure. The options of treatment include intravenous (IV) steroids, oral steroids, adrenocorticotropic hormone (ACTH), plasma exchange, disease-modifying treatments (DMTs), and nonpharmacologic modalities, such as physical therapy.
Treatment for an MS relapse is initially 1,000 mg of methylprednisolone IV or orally daily for three to five days.63 A three-day course has fewer side effects compared to the five-day course. Inform the patient about the side effects of methylprednisolone that include facial flushing, dysgeusia, hyperglycemia, gastrointestinal upset, elevated blood pressure, insomnia, anxiety or agitation, hypokalemia, and peripheral edema. Consider providing prophylactic prescribed or over-the-counter medications to mitigate these side effects (e.g., a proton pump inhibitor or sucralfate and metoclopramide for gastrointestinal symptoms).64 Oral steroids may be preferred over IV, since they are less cumbersome, less expensive, and appear to be equally as effective as IV.65 The dosing of oral steroids is 25 50-mg prednisone tablets or 32 6-mg dexamethasone tablets per day for three to five days. Intravenous corticosteroids have been the standard treatment in the past for optic neuritis, but there is recent evidence that oral corticosteroids are not inferior to IV steroids for optic neuritis.66 Steroids typically alleviate symptoms within one week. If there is no improvement by two weeks, this is considered a treatment failure.67,68 If there is no improvement, patients can receive a second course of steroids, ACTH, or plasma exchange.68-71
Treating true relapses with high-dose corticosteroids mitigates inflammation leading to a reduction in new neurologic deficits. True relapses should be suspected with a new neurologic territory impairment. This diagnosis can be made clinically and does not always require an MRI, although further imaging may be considered in the ED in consultation with the patient’s neurologist.
When a pseudorelapse is diagnosed, treat the underlying cause. Avoid steroids in patients who present with a pseudorelapse, since steroids can be immunosuppressive, which may exacerbate underlying pathology. Evaluate for urinary tract infections, respiratory infections, and viral infections. Treat the underlying etiology of the pseudorelapse with appropriate antibiotics, antifungals, or antivirals as appropriate.
Treat fever with antipyretics, since increased body temperature worsens MS symptoms.72,73 Elucidate any difficulties with medication compliance, dosing schedule, or side effects, since noncompliance may lead to pseudorelapse as well.
Consider and counsel selected patients on “needle fatigue,” which is a condition in MS patients that occurs when they stop taking DMTs (i.e., high-frequency interferon beta and glatiramer acetate) because of intolerable side effects from the injections, which can happen in 17% to 46% of those in their first year of treatment.74-76 Oral treatments or parenteral treatments that are given once every two weeks have been shown to be an effective alternative to improve compliance when needle fatigue is present.7
Nonpharmacologic modalities and patient preference of treatment should be based on acceptance and adherence by the patient. Options include exercise, nutritional counseling, psychosocial therapy, occupational therapy, physical therapy, and speech therapy, which have been demonstrated to improve outcomes in MS.77-79 This will improve the patient’s overall quality of life by improving the patient’s physical, mental, and social health.80 Recommending outdoor activity may be important also because sun exposure has protective effects against MS.81,82
Address modifiable risk behaviors that can reduce the relapse and/or progression of MS that include cessation of cigarette smoking, increased sun exposure, increased exercise, Mediterranean diets, reduced exposure to air pollution, and weight loss in obese patients.17
MS relapses often will improve spontaneously or resolve without medications. Therefore, after a careful discussion with the patient and his/her neurologist, patients may opt to forego initiation or alterations in medications. Shared decision-making is important to deliver good and compliant care.
Disposition
Unless the patient otherwise meets inpatient criteria, outpatient management in a patient with an MS relapse is preferred for cost savings, patient wellness, and avoidance of overtreating.83
Inpatient criteria can be considered in patients with suspected new-onset MS. An admission may be indicated to evaluate whether the patient is presenting with MS vs. a non-MS diagnosis, such as a stroke. An MS workup can include MRIs and neurology consultation as well as possible LP for CSF analysis and further laboratory tests. A neurologist will establish the diagnosis of MS.
Outpatient workup can be considered if the patient can follow up soon and demonstrates good compliance, and if urgent outpatient MRI testing and neurology consultation are available. Outpatient treatment of a relapse or a pseudorelapse (e.g., infection) also should include the clinical stability or functional safety of the outpatient setting. Evaluate the patient’s ability to care for himself or herself and the need for IV medications, oxygen, physical therapy, or other inpatient medical interventions that are required. If the patient is stable to be discharged, involve the consultation of a neurologist to assist with an outpatient treatment plan and ensure close outpatient follow-up. When discharging the patient from the ED, make the patient aware of the various treatment options, adverse effects, drug interactions, compliance, identification of treatment failures, evaluation of readiness to initiate treatment, and barriers to treatment, and counsel patients on fertility and reproduction-related concerns.73
Summary
MS is a complex disease that often is challenging to diagnose and initiate management in the ED. Patients who have been previously diagnosed with MS often will be knowledgeable about their condition, treatments, and disposition management. Many diagnostic considerations must be weighed when an MS patient presents to the ED, including differentiating between a new-onset presentation of MS, a relapse, and a pseudorelapse, which will guide the workup and disposition. Development of new neurologic signs or symptoms also may be a non-MS problem. Therefore, it is important that the emergency physician performs a careful history and physical exam and is familiar with the various presentations of MS, MS mimics, and conditions that can exacerbate the MS disease course. In addition to good communication, patient counseling and shared decision-making are important aspects of high-quality care. Each presentation will require a thorough evaluation and workup, patient involvement, neurology consultation, and a disposition and management plan that addresses the patient’s unique circumstances. As imaging technology advances, new pharmacologic and non-pharmacologic therapies are developed, and protocols evolve, high-quality outcomes in MS depend on a well-informed emergency physician.
REFERENCES
- Farber R, Hannigan C, Alcauskas M, Krieger S. Emergency department visits before the diagnosis of MS. Mult Scler Relat Disord 2014;3:350-354.
- Noyes K, Weinstock-Guttman B. Impact of diagnosis and early treatment on the course of multiple sclerosis. Am J Manag Care 2013;19(17 Suppl):s321-s331.
- Lublin FD, Reingold SC, Cohen JA, et al. Defining the clinical course of multiple sclerosis: The 2013 revisions. Neurology 2014;83:278-286.
- Miller DH, Chard DT, Ciccarelli O. Clinically isolated syndromes. Lancet Neurol 2012;11:157-169.
- Zeydan B, Kantarci OH. Impact of age on multiple sclerosis disease activity and progression. Curr Neurol Neurosci Rep 2020;20:24.
- Amato MP, Fonderico M, Portaccio E, et al. Disease-modifying drugs can reduce disability progression in relapsing multiple sclerosis. Brain 2020;143:3013-3024.
- Thompson AJ, Baranzini SE, Geurts J, et al. Multiple sclerosis. Lancet 2018;391:1622-1636.
- Vidal-Jordana A, Montalban X. Multiple sclerosis: Epidemiologic, clinical, and therapeutic aspects. Neuroimaging Clin N Am 2017;27:195-204.
- Wallin MT, Culpepper WJ, Campbell JD, et al. The prevalence of MS in the United States: A population-based estimate using health claims data. Neurology 2019;92:e1029-e1040. [Published correction appears in Neurology 2019;93:688.]
- Yamasaki R, Kira J. Multiple sclerosis. In: Sango K, Yamauchi J, Ogata T, Susuki K, eds. Myelin: Basic and Clinical Advances. Springer; 2019.
- Leray E, Moreau T, Fromont A, Edan G. Epidemiology of multiple sclerosis. Rev Neurol (Paris) 2016;172:3-13.
- Thompson AJ, Banwell BL, Barkhof F, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol 2018;2:162-173.
- Compston A, McDonald IR, Noseworthy J, et al, eds. McAlpine’s Multiple Sclerosis, 4th ed. Churchill Livingstone; 2005.
- Hirst C, Ingram G, Pickersgill T, et al. Increasing prevalence and incidence of multiple sclerosis in South East Wales. J Neurol Neurosurg Psychiatry 2009;80:386-391.
- Miller DH, Leary SM. Primary-progressive multiple sclerosis. Lancet Neurol 2007;6:903-912.
- Belbasis L, Bellou V, Evangelou E, et al. Environmental risk factors and multiple sclerosis: An umbrella review of systematic reviews and meta-analyses. Lancet Neurol 2015;14:263-273.
- Waubant E, Lucas R, Mowry E, et al. Environmental and genetic risk factors for MS: An integrated review. Ann Clin Transl Neurol 2019;6:1905-1922.
- Laribi B, Shekarabi M, Zarnani AH, et al. Differential serostatus of Epstein-Barr virus in Iranian MS patients with various clinical patterns. Med J Islam Repub Iran 2018;32:118.
- Houen G, Trier NH, Frederiksen JL. Epstein-Barr virus and multiple sclerosis. Front Immunol 2020;11:587078.
- Wasko NJ, Nichols F, Clark RB. Multiple sclerosis, the microbiome, TLR2, and the hygiene hypothesis. Autoimmun Rev 2020;19:102430.
- Smith KJ, McDonald WI. The pathophysiology of multiple sclerosis: The mechanisms underlying the production of symptoms and the natural history of the disease. Philos Trans R Soc Lond B Biol Sci 1999;354:1649-1673.
- Margolin E. The swollen optic nerve: An approach to diagnosis and management. Pract Neurol 2019;19:302-309.
- Henderson AP, Altmann DR, Trip SA, et al. Early factors associated with axonal loss after optic neuritis. Ann Neurol 2011;70:955-963.
- Nij Bijvank JA, van Rijn LJ, Balk LJ, et al. Diagnosing and quantifying a common deficit in multiple sclerosis: Internuclear ophthalmoplegia. Neurology 2019;92:e2299-e2308.
- Brassington JC, Marsh NV. Neuropsychological aspects of multiple sclerosis. Neuropsychol Rev 1998;8:43-77.
- Rao SM. Neuropsychology of multiple sclerosis. Curr Opin Neurol 1995;8:216-220.
- Ciccarelli O, Cohen JA, Reingold SC, et al. International Conference on Spinal Cord Involvement and Imaging in Multiple Sclerosis and Neuromyelitis Optica Spectrum Disorders. Spinal cord involvement in multiple sclerosis and neuromyelitis optica spectrum disorders. Lancet Neurol 2019;18:185-197.
- Rodríguez de Antonio LA, García Castañón I, Aguilar-Amat Prior MJ, et al. Non-inflammatory causes of emergency consultation in patients with multiple sclerosis. Neurología 2021;36:403-411.
- Kalincik T, Buzzard K, Jokubaitis V, et al. Risk of relapse phenotype recurrence in multiple sclerosis. Mult Scler 2014;20:1511-1522.
- Mahadeva A, Tanasescu R, Gran B. Urinary tract infections in multiple sclerosis: Under-diagnosed and under-treated? A clinical audit at a large University Hospital. Am J Clin Exp Immunol 2014;3:57-67.
- Sakakibara R. Neurogenic lower urinary tract dysfunction in multiple sclerosis, neuromyelitis optica, and related disorders. Clin Auton Res 2019;29:313-320.
- Guan XL, Wang H, Huang HS, Meng L. Prevalence of dysphagia in multiple sclerosis: A systematic review and meta-analysis. Neurol Sci 2015;36:671-681.
- Davis SL, Jay O, Wilson TE. Thermoregulatory dysfunction in multiple sclerosis. Handb Clin Neurol 2018;157:701-714.
- Tzelepis GE, McCool FD. Respiratory dysfunction in multiple sclerosis. Respir Med 2015;109:671-679.
- Howard RS, Wiles CM, Hirsch NP, et al. Respiratory involvement in multiple sclerosis. Brain 1992;115:479-494.
- Perez CA, Smith A, Nelson F. Multiple Sclerosis, A Practical Manual for Hospital and Outpatient Care. Cambridge University Press. March 2021.
- Taus C, Giuliani G, Pucci E, et al. Amantadine for fatigue in multiple sclerosis. Cochrane Database Syst Rev 2003;(2):CD002818.
- Witenko C, Moorman-Li R, Motycka C, et al. Considerations for the appropriate use of skeletal muscle relaxants for the management of acute low back pain. P T 2014;39:427-435.
- Benedict RH, Munschauer, F, Zarevics P, et al. Effects of l-amphetamine sulfate on cognitive function in multiple sclerosis patients. J Neurol 2008;255:848.
- Benedict RHB, Cookfair D, Gavett R, et al. Validity of the minimal assessment of cognitive function in multiple
sclerosis (MACFIMS). J Int Neuropsychol Soc 2006;12:549-558. - Olivares T, Nieto A, Sánchez MP, et al. Pattern of neuropsychological impairment in the early phase of relapsing-remitting multiple sclerosis. Mult Scler 2005;11:191-197.
- Brenner P, Piehl F. Fatigue and depression in multiple sclerosis: Pharmacological and non-pharmacological interventions. Acta Neurol Scand 2016;134(Suppl 200):47-54.
- Barker AB, Lincoln NB, Hunt N, dasNair R. Social identity in people with multiple sclerosis: An examination of family identity and mood. Int J MS Care 2018;20:85-91.
- Berzins SA, Bulloch AG, Burton JM, et al. Determinants and incidence of depression in multiple sclerosis: A prospective cohort study. J Psychosom Res 2017;99:169-176.
- Pérez Martín MY, González-Platas M, María Pilar PT. Perception of the disease in patients with multiple sclerosis.J Neur Diseases 2019;405:303.
- Bruce JM, Hancock LM, Arnett P, Lynch S. Treatment adherence in multiple sclerosis: Association with emotional status, personality, and cognition. J Behav Med 2010;33:219-227.
- Marrie RA, Zhang L, Lix LM, et al. The validity and reliability of screening measures for depression and anxiety disorders in multiple sclerosis. Mult Scler Relat Disord 2018;20:9-15.
- Kroenke K, Spitzer RL, Williams JBW. The Patient Health Questionnaire-2: Validity of a two-item depression screener. Med Care 2003;41:1284-1292.
- Fischer JS. Cognitive impairment in multiple sclerosis. In: Cook SD, ed. Handbook of Multiple Sclerosis. Marcel Dekker;2001:233-256.
- Mantero V, Abate L, Balgera R, et al. Clinical application of 2017 McDonald diagnostic criteria for multiple sclerosis. J Clin Neurol 2018;14:387-392.
- Barkhof F, Hommes OR, Scheltens P, Valk J. Quantitative MRI changes in gadolinium DTPA enhancement after high-dose intravenous methylprednisolone in multiple sclerosis. Neurology 1991;41:1219-1222.
- Zivadinov R, Rudick RA, De Masi R, et al. Effects of IV methylprednisolone on brain atrophy in relapsing-remitting MS. Neurology 2001;9:1239-1247.
- Zivadinov R, Zorzon M, De Masi R, et al. Effect of intravenous methylprednisolone on the number, size and confluence of plaques in relapsing-remitting multiple sclerosis. J Neurol Sci 2008;267:28-35.
- Brownlee WJ, Hardy TA, Fazekas F, Miller DH. Diagnosis of multiple sclerosis: Progress and challenges. Lancet 2017;389:1336-1346.
- Mahajan KR, Ontaneda D. The role of advanced magnetic resonance imaging techniques in multiple sclerosis clinical trials. Neurotherapeutics 2017;14:905-923.
- Sombekke MH, Wattjes MP, Balk LJ, et al. Spinal cord lesions in patients with clinically isolated syndrome: A powerful tool in diagnosis and prognosis. Neurology 2013;80:69-75.
- Bot JCJ, Barkhof F, Lycklama à Nijeholt G, et al. Differentiation of multiple sclerosis from other inflammatory disorders and cerebrovascular disease: Value of spinal MR imaging. Radiology 2002;223:46-56.
- Fisniku LK, Brex PA, Altmann DR, et al. Disability and T2 MRI lesions: A 20-year follow-up of patients with relapse onset of multiple sclerosis. Brain 2008;131:808-817.
- Dobson R, Ramagopalan S, Davis A, Giovannoni G. Cerebrospinal fluid oligoclonal bands in multiple sclerosis and clinically isolated syndromes: A meta-analysis of prevalence, prognosis and effect of latitude. J Neurol Neurosurg Psychiatry 2013;84:909-914.
- Solomon AJ, Weinshenker BG. Misdiagnosis of multiple sclerosis: Frequency, causes, effects, and prevention. Curr Neurol Neurosci Rep 2013;13:403.
- Solomon AJ, Klein EP, Boudette D. “Undiagnosing” multiple sclerosis: The challenge of misdiagnosis in MS. Neurology 2012;78:1986-1991.
- Castelo-Branco A, Chiesa F, Conte S, et al. Infections in patients with multiple sclerosis: A national cohort study in Sweden. Mult Scler Relat Disord 2020;45:102420.
- Tremlett HL, Luscombe DK, Wiles CM. Use of corticosteroids in multiple sclerosis by consultant neurologists in the United Kingdom. J Neurol Neurosurg Psychiatry 1998;65:362-365.
- Chataway J, Porter B, Riazi A, et al. Home versus outpatient administration of intravenous steroids for multiple-sclerosis relapses: A randomised controlled trial. Lancet Neurol 2006;5:565-571.
- Le Page E, Veillard D, Laplaud DA, et al. Oral versus intravenous high-dose methylprednisolone for treatment of relapses in patients with multiple sclerosis (COPOUSEP): A randomised, controlled, double-blind, non-inferiority trial. Lancet 2015;386:974-981.
- Morrow SA, Fraser JA, Day C, et al. Effect of treating acute optic neuritis with bioequivalent oral vs intravenous corticosteroids: A randomized clinical trial. JAMA Neurol 2018;75:690-696.
- Stoppe M, Busch M, Krizek L, Then Bergh F. Outcome of MS relapses in the era of disease-modifying therapy. BMC Neurol 2017;17:10-17.
- Weinshenker BG, O’Brien PC, Petterson TM, et al. A randomized trial of plasma exchange in acute central nervous system inflammatory demyelinating disease. Ann Neurol 1999;46:878-886.
- Keegan M, Pineda AA, McClelland RL, et al. Plasma exchange for severe attacks of CNS demyelination: Predictors of response. Neurology 2002;58:143-146.
- Cortese I, Chaudhry V, So YT, et al. Evidence-based guideline update: Plasmapheresis in neurologic disorders. Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 2011;76,3:294-300.
- Flanagan EP. Neuromyelitis optica spectrum disorder and other non-multiple sclerosis central nervous system inflammatory diseases. Continuum 2019;25:815-844.
- Ontaneda D, Rae-Grant AD. Management of acute exacerbations in multiple sclerosis. Ann Indian Acad Neurol 2009;12:264-272.
- Rae-Grant A, Day GS, Marrie RA, et al. Practice guideline recommendations summary: Disease-modifying therapies for adults with multiple sclerosis: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 2018;90:777-788
- McKay KA, Tremlett H, Patten SB, et al. Determinants of nonadherence to disease-modifying therapies in multiple sclerosis: A cross-Canada prospective study. Mult Scler 2017;23:588-596.
- Clerico M, Barbero P, Contessa G, et al. Adherence to interferon-beta treatment and results of therapy switching. J Neurol Sci 2007;259:104-108.
- Tan H, Cai Q, Agarwal S, et al. Impact of adherence to disease-modifying therapies on clinical and economic outcomes among patients with multiple sclerosis. Adv Ther 2011;28:51-61.
- National Institute for Health and Care Excellence (UK). NICE Clinical Guidelines, No. 186. Multiple Sclerosis: Management of multiple sclerosis in primary and secondary care. National Institute for Health and Care Excellence; 2014.
- McNicholas N, Lockhart A, Yap SM, et al. New versus old: Implications of evolving diagnostic criteria for relapsing-remitting multiple sclerosis. Mult Scler 2019;25:867-870.
- Craig J, Young CA, Ennis M, et al. A randomised controlled trial comparing rehabilitation against standard therapy in multiple sclerosis patients receiving intravenous steroid treatment. J Neurol Neurosurg Psychiatry 2003;74:1225-1230.
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour. World Health Organization; 2020.
- Tremlett H, Zhu F, Ascherio A, Munger KL. Sun exposure over the life course and associations with multiple sclerosis. Neurology 2018;90:e1191-e1199.
- Espinosa-Ramírez G, Ordoñez G, Flores-Rivera J, Sotelo J. Sunlight exposure and multiple sclerosis in a tropical country. Neurol Res 2014;36:647-650.
- Abboud H, Mente K, Seay M, et al. Triaging patients with multiple sclerosis in the emergency department: Room for improvement. Int J MS Care 2017;19:290-296.