Nonalcoholic Fatty Liver Disease
AUTHORS
Kim Pfotenhauer, DO, Assistant Professor, Touro University California College of Osteopathic Medicine (TUCCOM), Vallejo, CA
Clipper F. Young, PharmD, MPH, CDE, BC-ADM, Assistant Professor and Clinical Pharmacist, Primary Care Department, Touro University California, Vallejo, CA
Joy Dugan, PA-C, MPH, Assistant Program Director, Joint MSPAS/MPH Program, Touro University California, Vallejo, CA
Jay H. Shubrook, DO, Professor, TUCCOM, Vallejo, CA
PEER REVIEWER
Charlie Abraham, MD, MBA, FACP, Clinical Assistant Professor, UCSF-Fresno
Nonalcoholic fatty liver disease (NAFLD) is the most common liver pathology worldwide.1 The increase in obesity and insulin resistance has contributed to the disease burden. A continuum of fatty liver to hepatic steatosis to possible fibrosis, cirrhosis, or hepatocellular carcinoma, NAFLD is the third leading cause of liver transplantation in the United States.2 Even more alarming, this disease is expected to grow, as an estimated 10% of children in the United States have NAFLD.3
Nonalcoholic fatty liver disease is the presence of excessive fat accumulation in the liver and associated insulin resistance. This is defined as the presence steatosis in > 5% of hepatocytes by histological analysis or > 5.6% assessed by nuclear magnetic resonance techniques and no competing cause for the steatosis.4 As the name implies, the exclusion of recent or ongoing alcohol consumption as a mechanism for steatosis (defined as > 21 drinks per week for men and > 14 drinks per week for women) is necessary.4 NAFLD is characterized further based on histology. Nonalcoholic fatty liver (NAFL) is having no evidence of hepatocellular injury although there is hepatic steatosis.4 Nonalcoholic steatohepatitis (NASH) is the “presence of hepatic steatosis and inflammation with hepatocyte injury with or without fibrosis.”4 This article reviews the pathogenesis, diagnosis, and natural history of NAFLD as well as known treatments and future therapies.
Epidemiology
The true prevalence of NAFLD/NASH is difficult to determine, as the condition often is silent. Often, patients progress without obtaining a specific diagnosis. Many people are unaware that they have this condition until they decompensate from cirrhosis. That being said, the spectrum of fatty liver disease has grown rapidly around the world and has been called a global epidemic.5 It is estimated that the global incidence of NAFLD is 5-38%, with a NASH incidence of 20-30% in Western countries and 5-18% in Asia.6
Rates of NAFLD are higher in men than women but the difference diminishes after menopause.7 However, women are also more likely to suffer complications from fatty liver disease.7
There are ethnic differences in the rates of NAFLD and its complications. In the Dallas Heart study, the general rate of NAFLD was 31%, with Hispanics having a rate of 45%, Caucasians 33%, and black Americans 24%.8 Despite Hispanics having high rates of NAFLD, they are less likely to progress to advanced disease.9 Specifically, Hispanics who are homozygous for the PNPLA3 allele (patatin-like phospholipase domain-containing protein 3 rs73809) have twice the hepatic fat content.10 It also appears that Asians are more likely to suffer from advanced disease and complications from NAFLD.11
Recently, there is the emergence of fatty liver in children. It has been estimated that fatty liver disease is the most common liver abnormality found in children ages 2 to 19 years.12 With increases in childhood obesity and more than two-thirds of adults currently overweight or obese, the burden of NAFLD and its complications surely will increase over the next generation. This likely will make NASH and its complications the next obesity-related epidemic. Many more people are at risk for developing cirrhosis and hepatocellular cancer.13
Pathogenesis
NAFLD is a spectrum of disorders, all of which share abnormal deposition of fat into the hepatic parenchyma. A key abnormality in NAFLD is the deregulation of insulin-mediated control of hepatic glucose and lipid production. This sets the stage for all that follows. The spectrum of NAFLD can be steatosis in the liver to steatohepatitis, which has been linked to bridging fibrosis, cirrhosis, and hepatocellular cancer. The central problem is an imbalance of how triglycerides are handled metabolically. Most triglycerides are not from the diet but rather from the breakdown of visceral fat (lipolysis) and the production of new fat from the liver (de novo lipogenesis).14 The triglycerides are broken into free fatty acids, which in turn initiate an inflammatory cascade via oxidative stress and adipokines.15
Researchers agree that there are both genetic and environmental contributions to NAFLD and that there are multiple abnormal processes in play in this disease. These is a “multi-hit hypothesis” that appears to be most plausible.5 First, there is an increase in hepatic intracellular fat that is seen in insulin resistance and contributes to more insulin resistance. This will increase the inflammatory response, which may lead to hepatocellular damage and further contribute to insulin resistance. The lipid oxidation and release of reactive oxidative species induces further damage. Later, as part of the repair process, ballooning and fibrosis can occur.
A number of new developments have been elucidated in the pathophysiology of NAFLD. Now it is believed that the initial development of NAFLD can begin in utero.16 This is particularly true in obese mothers or those with type 2 diabetes. The PNPLA3 is tied most closely to the development of NAFLD and is seen in times of excessive food intake, particularly in Hispanic patients. Specifically, the presence of the PNPLA3 allele was associated with a higher likelihood of fibrosis.17 (See Figure 1.)
Figure 1. Pathophysiological Mechanisms Linking Obesity, Nonalcoholic Fatty Liver Disease, Cardiovascular Disease, Chronic Kidney Disease, and Diabetes Mellitus Type 2 |
 |
|
NAFLD: nonalcoholic fatty liver disease; RAAS: renin-angiotensin-aldosterone system Adapted with permission from: Mikolasevic I, et al. Nonalcoholic fatty liver disease — A multisystem disease? World J Gastroenterol 2016;22:9492. |
It is important to remember that not all people diagnosed with NASH will progress. It is estimated that 20% actually will see a regression of their disease. However, 33% will progress to fibrosis and cirrhosis.13
Staging of NAFLD is based on percentage of hepatic steatosis. Less than 5% steatotic involvement is considered physiological. Pathologic steatosis is divided into three stages: 5-33% (mild), 35-66% (moderate), and > 66% (severe).18
There are a number of systems to “grade” or “stage” NAFLD. These include the Brunt system;18 the steatosis, activity, and scoring system;19 and the NASH clinical research network NAFLD activity score.20 (See Tables 1, 2, and 3.)
Table 1. Nonalcoholic Fatty Liver Disease Activity Scoring System |
|
|
Steatosis, grade (0-3) |
|
|
< 5% |
0 |
|
5-33% |
1 |
|
34-66% |
2 |
|
> 66% |
3 |
|
Lobular inflammation |
|
|
No foci |
0 |
|
< 2 foci per 200 × field |
1 |
|
2-4 foci per 200 × field |
2 |
|
> 4 foci per 200 × field |
3 |
|
Hepatocyte ballooning |
|
|
None |
0 |
|
Few balloon cells |
1 |
|
Many cells/prominent ballooning |
2 |
|
Fibrosis stage |
|
|
None |
0 |
|
Perisinusoidal or periportal |
1 |
|
Mild, zone 3, perisinusoidal |
1A |
|
Moderate, zone 3, perisinusoidal |
1B |
|
Portal/periportal |
1C |
|
Perisinusoidal and portal/periportal |
2 |
|
Bridging fibrosis |
3 |
|
Cirrhosis |
4 |
|
Adapted with permission from: Benedict M, Zhang X. Non-alcoholic fatty liver disease: An expanded review. World J Hepatol 2017;9:722. |
|
Table 2. Steatosis, Activity, and Fibrosis Scoring System |
|
Steatosis score (S): Assessed the quantities of large or medium-sized lipid droplets (0-3) |
|
S0: < 5% |
|
S1: 5-33% |
|
S2: 34-66% |
|
S3: > 67% |
|
Activity grade (0-4): Sum of scores for ballooning and lobular inflammation |
|
A1: Mild activity |
|
A2: Moderate activity |
|
A3 and A4: Severe activity |
|
Hepatocyte ballooning (0-2) |
|
0: None |
|
1: Foci of hepatocytes with rounded shape, pale or reticulated cytoplasm |
|
2: Foci of hepatocytes with rounded shape, pale or reticulated cytoplasm, and enlargement (> 2 × normal size) |
|
Lobular inflammation (0-2) |
|
0: None |
|
1: < 2 foci per 20 × field |
|
2: < 2 foci per 20 × field |
|
Fibrosis stage (F) |
|
F0: No relevant fibrosis |
|
F1: 1a - mild zone 3 perisinusoidal fibrosis 1b - moderate zone 3 perisinusoidal fibrosis 1c - portal fibrosis |
|
F2: Zone 3 perisinusoidal fibrosis with periportal fibrosis |
|
F3: Bridging fibrosis |
|
F4: Cirrhosis |
|
Adapted with permission from: Benedict M, Zhang X. Non-alcoholic fatty liver disease: An expanded review. World J Hepatol 2017;9:722. |
Table 3. Brunt Grading and Staging of Nonalcoholic Steatohepatitis |
|
|
Grading |
Staging |
|
Mild (Grade 1)
|
Stage 1 Zone 3 perisinusoidal/pericellular fibrosis (focal or extensive) |
|
Moderate (Grade 2)
|
Stage 2 Zone 3 perisinusoidal/pericellular fibrosis with associated focal or extensive periportal fibrosis |
|
Severe (Grade 3)
|
Stage 3 Zone 3 perisinusoidal/pericellular fibrosis and portal fibrosis with associated focal or extensive bridging fibrosis |
|
Stage 4 Cirrhosis |
|
|
Adapted with permission from: Benedict M, Zhang X. Non-alcoholic fatty liver disease: An expanded review. World J Hepatol 2017;9:723. |
|
NAFLD is a systemic disease, and has been shown to be a risk factor for other diseases, such as colorectal cancer, chronic kidney disease, cardiovascular disease, type 2 diabetes, and psoriasis.15
NAFLD and Metabolic Syndrome
NAFLD should be considered as part of the metabolic syndrome. People with NAFLD meet criteria for metabolic syndrome and are more likely to have prediabetes or type 2 diabetes, polycystic ovarian disease, and obstructive sleep apnea.15 People with type 2 diabetes typically have 80% more hepatic fat than those without diabetes, even when matched for gender, age, and weight. Further, they are two to four times more likely to suffer from fatty liver-induced complications.7
NAFLD and Type 2 Diabetes
This risk of developing type 2 diabetes is increased almost five-fold in the presence of NAFLD.21 It has been harder to determine if those with type 2 diabetes have a higher risk of NAFLD. However, there is an increased risk of chronic kidney disease, retinopathy, and increased insulin requirements in the setting of both NAFLD and type 2 diabetes.21 The mortality from cirrhosis was increased significantly in those with NAFLD and type 2 diabetes in one large cohort study.22
Mechanisms in NAFLD and CVD
Numerous trials have shown that NAFLD is an independent predictor of adverse cardiovascular events. In addition to inflammation, one of the proposed mechanisms is excessive use of endothelial progenitor cells, which are believed to try to repair endothelial damage but also contribute to worsening of lipid abnormalities. Further, increased hepatic fat reduces adiponectin secretion, which is protective by reducing thrombus and atherosclerosis. Finally, leptin is increased in NAFLD, which will increase fat deposition in the liver.
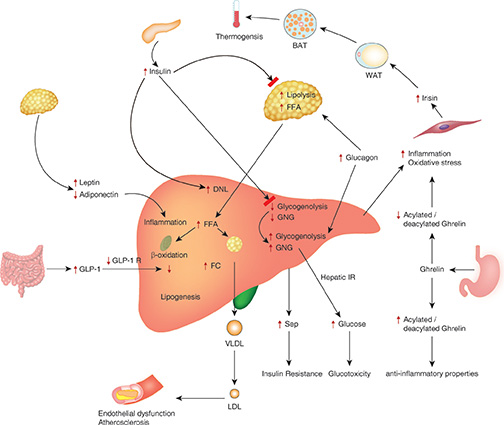
A person is likely at genetic risk for NAFLD and then dysfunctional fatty tissue contributes to an increase in systemic oxidative stress and inflammatory markers. This can lead to insulin resistance, which further feeds back to fatty liver dysfunction. There also appears to be “cross talk” about visceral and organ fat tissues including hepatic fat adipose tissue. (See Figure 2.)
Figure 2. Pathophysiological Mechanisms Involved in the Development and Complications of Nonalcoholic Fatty Liver Disease |
 |
|
BAT: brown adipose tissue; DNL: de novo lipogenesis; FC: free cholesterol; FFA: free fatty acid; GLP-1: glucagon-like insulinotropic peptide; Reprinted with permission from: Pappachan JM, et al. Non-alcoholic fatty liver disease: A clinical update. J Clin Translat Hepatol 2017;5:386. |
Natural History
NAFLD usually progresses slowly. However, rapid fibrosis is present in up to 20% of cases. In general, there is a rate of progression of one fibrosis stage for every 14 years in NAFL vs. every seven years in NASH.23 Although no increased rate exists for ultrasound-diagnosed NAFLD, there is an increased mortality for those with NASH. The risk of all-cause mortality increases when fibrosis is present and is higher with advancing stage of fibrosis.24 Cardiovascular disease, cancer, and liver disease are the most common causes of death for those with NASH.23
There is some evidence that NAFLD may lead to increased risk in hepatocellular carcinoma.23 Less systematic surveillance has led to NAFLD-associated hepatocellular carcinoma often being diagnosed at a more advanced stage.23
Risk Factors
Conditions that are associated with insulin resistance put patients at higher risk for NAFLD. These include obesity, type 2 diabetes, dyslipidemia, and metabolic syndrome. Also, several conditions have an emerging association with NAFLD, including polycystic ovary syndrome, hypothyroidism, obstructive sleep apnea, hypopituitarism, hypogonadism, and pancreato-duodenal resection.4 There is some evidence that cholecystectomy may be a risk factor for NAFLD. A study of 12,232 patients from the third U.S. National Health and Nutrition Examination Survey, 1988-1994, looked at patients who had ultrasonography for gallstone disease. Those with a history of cholecystectomy had a higher prevalence of NAFLD than those with gallstones.25
Certain conditions also increase the likelihood of progression to NASH or cirrhosis. Type 2 diabetes, metabolic syndrome, severe insulin resistance, tobacco use, weight gain of > 5 kg, and rising serum AST and ALT levels increase the risk of progression to NASH.26 In studies of patients with type 2 diabetes, between 69-87% of individuals had NAFLD.27,28 Those with NAFLD also commonly have dyslipidemia with high serum triglyceride levels and low serum high-density lipoprotein levels.29 In patients undergoing bariatric surgery, histologic evidence of NAFLD was as high as 90%, with 5% having unsuspected cirrhoisis.30
Screening
Currently, the American Gastroenterological Association does not recommend asymptomatic screening because of the high costs of testing, the risk of liver biopsy, and the deficit in definitive treatment.4 However, a joint statement from the European Association for the Study of the Liver, European Association for the Study of Diabetes, and the European Association for the Study of Obesity recommends screening those populations that are at risk for NAFLD.23 It is recommended that those with obesity or metabolic syndrome be screened by liver enzymes and/or ultrasound. This group further recommends screening high-risk individuals (age > 50 years, type 2 diabetes, or metabolic syndrome) for NASH, as they are at a higher risk for advanced disease.23
Clinical Manifestations
The vast majority of patients with NAFLD are asymptomatic. Patients with NASH are more likely to have complaints of fatigue and right upper abdominal discomfort. On physical exam, patients with NAFLD may have hepatomegaly. In an Indian study of 1,168 patients, 5% of patients had palpable hepatomegaly.31 If patients progress to cirrhosis, they may have weight loss, palmar erythema, spider angiomas, jaundice, ascites, and edema. Up to 90% of patients may have acanthosis nigricans on physical exam due to the associated insulin resistance common in NAFLD.32 (See Table 4.)
Table 4. Symptoms and Signs of NAFLD |
|
Diagnosis
According the to American Gastroenterological Association, the diagnosis of NAFLD requires four criteria: 1) hepatic steatosis by imaging or histology, 2) no significant alcohol consumption, 3) no competing etiologies for hepatic steatosis, and 4) no coexisting causes for chronic liver disease.4 (See Table 5.)
Table 5. Criteria for Diagnosis of NAFLD |
|
Alcohol consumption, hepatitis C, medications, parenteral nutrition, Wilson’s disease, and severe malnutrition all should be considered as alternative causes of hepatic steatosis.4 Hemochromatosis, autoimmune liver disease, chronic viral hepatitis, and Wilson’s disease should be considered as alternative causes of chronic liver disease.4
Although screening currently is not recommended, the first indication for further investigation often is increased ALT and AST on routine labs. However, normal ALT and AST do not exclude NAFLD.33 Fatty liver commonly is found as an incidental finding on other imaging.
The gold standard of diagnosis and staging is liver biopsy.4 This is the only definitive way to distinguish NAFL from NASH, fibrosis, and cirrhosis. In those with an increased risk of steatohepatitis and advanced fibrosis, liver biopsy should be considered.4 Steatosis alone, steatosis with lobular or portal inflammation but without ballooning, or steatosis with ballooning but without inflammation are all diagnostic of NAFL.23 On liver biopsy, evidence of hepatocellular injury in the form of ballooning of hepatocytes and inflammation is indicative of NASH.4
Several less-invasive methods are being developed. FibroTest/FibroSure, Hepascore, FibroSpect, and APRI (aspartate aminotransferase [AST] to platelet ratio) are the panels that have been studied most often. Although these investigations are fairly sufficient at differentiating between patients with significant fibrosis and those without fibrosis, they cannot discriminate reliably between the different stages of fibrosis.34 (See Table 6.)
Table 6. Investigational Noninvasive Tests for NAFLD |
||
|
Test |
Diagnostic Criteria |
Benefits |
|
FibroTest/FibroSure |
Alpha-2-macroglobulin, alpha-2-globulin (haptoglobin), gamma globulin, apolipoprotein A1, GGT, total bilirubin, age, sex |
Grouped: Mild fibrosis (F0-F1) Significant fibrosis (F2-F4) Indeterminate stage of fibrosis Primarily studied in those with hepatitis B and C84 |
|
ActiTest |
Same criteria as FibroTest/FibroSure with the addition of ALT |
Improved identification of more advanced fibrosis85 |
|
Hepascore |
Bilirubin, GGT, hyaluronic acid, alpha-2-macroglobulin, age, sex |
More accurate for alcoholic liver disease and fibrosis in hepatitis C86 |
|
FIB-4 index |
Platelet count, ALT, AST, age |
Appears helpful in predicting outcomes in NAFLD87 |
|
NAFLD fibrosis score |
Age, BMI, blood glucose levels, aminotransferase levels, platelet count, albumin |
Positive predictive value for advanced fibrosis of 82% and low cutoff value associated with negative predictive value of 88%88 |
|
BARD Score |
BMI, AST/ALT ratio, presence of diabetes mellitus |
Positive predictive value of 69% and negative predictive value of 96%89 |
Current Treatment Options: Management
According to the American Association for the Study of Liver Disease (AASLD), the backbone for managing NAFLD should comprise treatment for liver disease as well as management for the underlying, associated metabolic comorbid conditions (i.e., obesity, hyperlipidemia, insulin resistance, and type 2 diabetes).35 Current treatment options include lifestyle modifications, bariatric surgery, and pharmacological agents. One of the AASLD treatment guidelines recommends that pharmacological agents used for improving liver disease should be reserved for those with biopsy-proven NASH and fibrosis, as patients with NAFLD without steatohepatitis or any degree of fibrosis — from the perspective of the liver — have good prognosis.35
Lifestyle Modifications
Like other chronic disease management, diet, physical activity, and weight loss have been demonstrated effective in treating NAFLD, especially weight loss. As little as a 5% reduction is the key for improving the histopathological features of NASH.36,37 A 3-5% weight loss is needed to improve steatosis, and a 7-10% weight loss is necessary for the improvement in the majority of the NASH histopathological features.31 A long-term diet plan with caloric restriction has been shown to benefit the mobilization of liver fat in addition to cardiovascular risk reduction.38 Studies have shown that a 30% caloric reduction or 750 to 1,000 kcals per day led to improvement in insulin resistance and hepatic steatosis.39,40
A combination of a caloric restriction diet and moderate-intensity physical activity would yield the highest rate of sustained weight loss over time, thus improving the management of NAFLD.35 Data have suggested that weekly physical activity of at least 150 minutes, consisting of moderate-intensity physical activities (i.e., playing tennis for at least 10 minutes, biking at a steady pace, carrying light loads) would provide the greatest value in the prevention of NAFLD progression.41,42 Exercise alone may help reduce hepatic steatosis, but improving histopathological features of the liver remains unclear with exercise alone.35
Bariatric Surgery
The two most common causes of mortality in NAFLD are cardiovascular disease and cancer. Bariatric surgery can improve long-term survival and also reduce comorbid conditions in most patients.43-46 Clinical and metabolic data collected via liver biopsies from several retrospective and prospective cohort studies have shown improvements in the severity of steatosis one year following a bariatric surgery (e.g., gastric band, bilio-intestinal bypass, and gastric bypass).35 Because of the lack of randomized controlled trials on bariatric surgery in treating NASH, it might be too early to consider foregut bariatric surgery as an established approach specifically to treat NAFLD; however, it can be an option for otherwise eligible obese patients with NAFLD.31 The safety, type, and efficacy of foregut bariatric surgery in managing NAFLD with established cirrhosis have not been well established.35
Pharmacological Agents
Currently, there are no FDA-approved pharmacological agents specifically for the management of NAFLD. Some of the medications used to treat and manage type 2 diabetes have been studied for their potential roles and benefits in managing NAFLD and NASH.
Metformin. Some studies have shown that metformin, which is an insulin sensitizer, improves serum aminotransferases and insulin resistance in patients with NASH, but this agent does not improve liver histology.47-49 Two meta-analyses that were conducted by Li et al and Musso et al confirmed that metformin did not lead to improvement in liver histology in NAFLD and NASH patients.50,51 Thus, for managing adult patients with NAFLD, the AASLD does not recommend metformin.35
Thiazolidinediones. These agents — rosiglitazone and pioglitazone — specifically bind to the nuclear transcription factor peroxisome proliferator-activated receptor gamma (PPAR-γ), exerting broad effects on glycemic control, lipid metabolism, vascular biology, and inflammation.52 Some studies have reported that rosiglitazone can improve hepatic steatosis but not necro-inflammation nor fibrosis.53,54 However, this agent remains severely restricted in use in the United States because of the controversial findings with a higher number of coronary events in the rosiglitazone group, although FDA did not confirm such association after reviewing all the evidence.55 Studies using pioglitazone in patients with NASH who were also managing prediabetes or type 2 diabetes have shown improvements in insulin sensitivity, aminotransferases, steatosis, and inflammation with trending toward fibrosis improvement.56,57 In patients with NASH without diabetes, pioglitazone also has been shown beneficial in reducing hepatocellular injuries and fibrosis.58 With results from numerous studies supporting its efficacy in improving liver histology, pioglitazone is recommended in patients with biopsy-proven NASH regardless of type 2 diabetes status.35 In patients without biopsy-proven NASH, pioglitazone is not recommended for the treatment of NAFLD until additional data supporting its safety and efficacy are available.35
Glucagon-like Peptide-1 (GLP-1) Receptor Agonists. Currently, the use of GLP-1 receptor agonists to treat patients with NAFLD or NASH is in the investigational stage. There have been some studies examining the potential effects of GLP-1 receptor agonists, mainly liraglutide and exenatide, in treating NAFLD and NASH.59-62 Results from two liraglutide studies have shown its safety and efficacy in improving liver function and histological features in NASH patients with type 2 diabetes.59,61 A randomized, placebo-controlled trial in patients using liraglutide once daily for 48 weeks demonstrated resolution of steatohepatitis and delay of the progression of fibrosis.60 More studies are necessary to confirm the role of GLP-1 receptor agonists in treating NAFLD or NASH.
Orlistat. The potential role of orlistat for treating NAFLD has been studied because of its indication in obesity management (through inhibiting lipase and preventing absorption of enteric lipid), supporting the overall weight-loss approach in treating this condition.63 A trial comparing orlistat and placebo in two groups of NASH patients who were also obese did not lead to a significant difference in weight loss. In addition to this agent, study participants in both groups were treated with vitamin E and dietary restriction.64 In the same study, when comparing results at the end of the trial to baseline data, improvements in insulin sensitivity, adiponectin, steatosis, inflammation, and NAS (NAFLD Activity Score) were observed in the study participants.64
Although reduction in liver enzymes and improvements in steatosis have been found in other orlistat trials, it was unclear whether the weight loss induced by orlistat could be sustained long-term.65 Additional clinical trials are needed to further explore the role of orlistat in the treatment of NAFLD/NASH.
Statins. Although statins are not recommended as the primary pharmacotherapy for treating NASH, patients with both NASH and dyslipidemia or cirrhosis may use a statin as part of their treatment plans.63 A study has shown an association between the use of a statin and a lower risk of hepatocellular cancer in those who had cirrhosis.66 In addition, there is no evidence linking the risk of liver injury and concurrent statin use in patients with NAFLD.67
Antioxidants
Vitamin E. As a free radical scavenger, vitamin E has been used to manage NAFLD/NASH, with the aim to reduce oxidative stress, which plays a crucial role in promoting the progression of NASH.68,69 In several studies, vitamin E has been shown to reduce serum hepatobiliary enzymes, hepatic inflammation, and steatosis in the liver.63 Thus, the AASLD recommends the use of vitamin E with a daily dose no more than 800 IU (because of its ability to improve liver histology) in adult patients without diabetes and with biopsy-proven NASH.35 The reason to keep the daily dose of vitamin E at 800 IU is because of a meta-analysis showing all-cause mortality increased with doses higher than 800 IU per day.70 When the decision is made to include vitamin E as part of the treatment plan, discussions with each patient about the risks and benefits of incorporating this agent are necessary before initiation. More data are needed to support the use of vitamin E in patients with diabetes and NASH, NAFLD without a liver biopsy, NASH cirrhosis, or cryptogenic cirrhosis.35
Future Pharmacological Therapies
Although there are no approved pharmacological agents yet for the treatment of NAFLD, there are many innovative approaches for the development of NAFLD/NASH pharmacotherapies, summarized in the following four pathways: 1) targeting hepatic fat accumulation; 2) reducing oxidative stress, inflammation, and apoptosis; 3) aiming intestinal microbiomes and metabolic endotoxemia; 4) antagonizing hepatic fibrosis.59 Various agents, such as obeticholic acid, elafobranor, selonsertib, and cenicriviroc, targeting these pathways are being studied in an international Phase III trial in treating NASH.59
Agents Targeting Hepatic Fat Accumulation
Elafobranor. Elafobranor is a dual agonist for PPAR-α/δ receptors, leading to results on improving steatosis, inflammation, and fibrosis in mice with NAFLD.72 It also has been shown in a Phase IIb trial to resolve NASH in patients with NAS ≥ 4 without aggravating hepatic fibrosis; in patients with NAS < 4, this agent has not been shown effective.73
Pemafibrate. A novel selective peroxisome proliferator-activated receptor alpha modulator (SPPARM-α), pemafibrate has been shown in a Phase II trial to reduce serum transaminase activities in patients with dyslipidemia.74 In a preclinical trial, this agent also has been demonstrated to enhance liver pathology in diet-restricted rodents with NASH,75 showing promise for a potential treatment for human NASH.
Obeticholic Acid (OCA). OCA is a ligand targeting farnesoid X receptor (FXR), leading to reduction of hepatic glucogenesis, lipogenesis, and steatosis in animals.71 There is also evidence demonstrating its ability to improve necro-inflammation in patients with NASH as well as to delay the progression of fibrosis.71,76
Aramchol. Aramchol is a cholic-arachidic acid conjugate, inhibiting the effects of stearoyl-CoA desaturase (SCD), thus halting de novo lipogenesis.71 In animal models, this agent has been shown to strongly lower hepatic fat accumulation.71 The same effect has been revealed in humans with a lower dose; thus, a current study with higher doses is being conducted in patients with biopsy-proven NASH (without cirrhosis).71,77
Agents Reducing Oxidative Stress, Inflammation, and Apoptosis
Selonsertib. Selonertib is an apoptosis signal-regulating kinase 1 (ASK 1) inhibitor; the activity of this enzyme has been reported to result in apoptosis and fibrosis initiated by extracellular TNF-α and intracellular oxidative stress.71,78 Thus, it has been proposed that inhibition of this enzyme might be a possible target in treating NASH.
Emricasan. In rodents, emricasan, an irreversible caspase inhibitor, improved NAS as well as fibrosis.79 The essential role of caspase is to initiate programmed cell death (e.g., apoptosis) and inflammation. There are some Phase IIb trials testing its safety and efficacy in patients with NASH.
Agents Aiming at Intestinal Microbiomes and Reducing Metabolic Endotoxemia
IMM-124e. IMM-124e is an IgG-rich extract from cow colostrum, specifically against lipopolysaccharide (LPS).71 This agent thus can be used to reduce the liver being exposed to gut-derived bacterial products/toxins and LPS.71 A Phase I/II trial enrolling 10 patients with biopsy-proven NASH has shown improvements in liver enzymes.80
Solithromycin. Solithromycin is a potent macrolide antibiotic that has been reported to reduce NAS in six patients with NASH in a Phase II trial after 90 days of treatment.71
Agents Antagonizing Hepatic Fibrosis
Cenicriviroc (CVC). CVC, which is a C-C motif chemokine receptor-2/5 (CCR2/5) antagonist, was developed primarily to reduce inflammation.71 This agent also elicits antifibrotic effects and reduces insulin resistance, as expected when antagonizing CCR2 would lead to improvements in glycemic control and when antagonizing CCR5 would harm collagen-producing hepatic steallate cells.71
Galectin-3 Antagonist. Expression of galectin-3 protein induces the progression of hepatic fibrosis; thus, its expression in macrophages nearby lipid-laden hepatocytes is increased in patients with NASH. A galectin antagonist, called GR-MD-02, has been revealed in mice to improve liver histology significantly by reducing collagen deposition and inflammation.81 Studies in humans are being conducted to establish this agent’s safety and efficacy profile.71
Although many investigational products still are being studied to ensure their safety and efficacy in humans, it still might be some time before patients with NAFLD/NASH truly can benefit from these innovative agents. It is hoped that in five years from now, patients with this condition will be able to choose from additional pharmacological options other than vitamin E and pioglitazone. To be included in the NAFLD/NASH treatment guidelines, cost-effectiveness and patient-focused benefits of these novel pharmacological agents are the key determining factors, as well as their safety and efficacy data. Although difficult to accomplish and maintain, lifestyle modifications, including dietary caloric restriction and physical activity leading to weight loss, have remained as the cornerstone approach in the management of NAFLD/NASH.
Patient Education
Educating patients about exercise and healthy diets is helpful for managing NAFLD and its associated comorbidities, including obesity, type 2 diabetes, and hyperlipidemia. The National Institute of Diabetes and Digestive and Kidney Diseases recommends a plant-based diet, plentiful in whole grains, fruit, and vegetables, for the treatment of NAFLD.82 Limiting fats, simple sugars, and fructose also is recommended.
The most important thing patients can do is lose weight. While they are focusing on small amounts of weight loss, the goal is to reduce visceral adiposity. This will require losing at least 5-10% of their excess body weight. There is evidence that weight loss can reduce progression of NAFLD and reverse progression of this disease.
Inform patients to avoid hepatoxins such as high doses of acetaminophen. Alcohol use should be monitored and patients should avoid heavy alcohol use, defined as more than four weeks of four drinks per day or more than 14 drinks per week for men. For women, heavy alcohol use is defined as more than three drinks per day or more than seven drinks per week.82 The American Liver Foundation has online support groups and patient education materials about NAFLD, NASH, and acute liver disease. Refer patients to this website (https://www.liverfoundation.org) for further information about NAFLD.83
SUMMARY
Overall, NAFLD is emerging as an epidemic. Adequate screening and noninvasive diagnostic criteria need to be developed to identify those most at risk. Although many treatment options are being investigated, there is still no definitive treatment besides weight loss and lifestyle changes.
REFERENCES
- Diehl AM, Day CD. Causes, pathogenesis, and treatment of nonalcoholic steatohepatitis. N Engl J Med 2017;377;21
- Zezos P, Renner E. Liver transplantation and non-alcoholic fatty liver disease. World J Gastroenterol 2014; 20:15532–15538.
- Baidal JW, et al. Associations of early to mid-childhood adiposity with elevated mid-childhood alanine aminotransferase levels in the project viva cohort. J Pediatrics 2018; doi: 10.1016/j.jpeds.2018.01.069.
- Chalasani N, et al. The diagnosis and management of non-alcoholic fatty liver disease: Practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Disease, and American College of Gastroenterology. Gastroenterol 2012;142:1592-1609.
- Benedict M, Zhang X. Nonalcoholic fatty liver disease: An expanded review. World J Heptatol 2017;9:715-732.
- Sayiner M, et al. Epidemiology of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis in the United States and the rest of the world. Clin Liver Dis 2016;20: 205-214.
- Lonardo A, et al. Epidemiological modifiers of non-alcoholic fatty liver disease: Focus on high-risk groups. Dig Liver Dis 2015;47:997-1006.
- Browning JD, et al. Prevalence of hepatic steatosis in an urban population in the United States: Impact of ethnicity. Hepatology 2004;40:1387-1095.
- Bambha K, et al. Ethnicity and nonalcoholic fatty liver disease. Hepatology 2012;55:769-780.
- Satapathy SK, Sanyal AJ. Epidemiology and natural history of nonalcoholic fatty liver disease. Semin Liver Dis 2015;35:221-235.
- Mohanty SR, et al. Influence of ethnicity on histological differences in non-alcoholic fatty liver disease. J Hepatol 2009;50:797-804.
- Schwimmer JB, et al. Prevalence of fatty liver in children and adolescents. Pediatrics 2006;118:1388-1393.
- Calzadilla Bertot L, Adams LA. The natural course of non-alcoholic fatty liver disease. Int J Mol Sci 2016;17:pii: E774.
- Donnelly KL, et al. Sources of fatty acids stored in liver and secreted via lipoproteins in patients with nonalcoholic fatty liver disease. J Clin Invest 2005;115:1343-1151.
- Mikolasevic I, et al. Nonalcoholic fatty liver disease: A multisystem disease? World J Gastroenterol 2016;21:9488-9505.
- Goyal NP, Schwimmer JB. The progression and natural history of pediatric nonalcoholic fatty liver disease. Clin Liver Dis 2016;20:325-338.
- Singal AG, et al. The effect of PNPLA3 on fibrosis progression and development of hepatocellular carcinoma: A meta-analysis. Am J Gastroenterol 2014;109:325-334.
- Brunt EM, et al. Nonalcoholic steatohepatitis: A proposal for grading and staging the histological lesions. Am J Gastroenterol 1999;94:2467-2474.
- Kleiner DE, et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005;41:1313-1321.
- Bedossa P, et al. Histopathological algorithm and scoring system for evaluation of liver lesions in morbidly obese patients. Hepatology 2012;56:1751-1759.
- Hazlehurst JM, et al. Non-alcoholic fatty liver disease and diabetes. Metabolism 2016;65:1096-1108.
- De Marco R, ET AL. Cause-specific mortality in type 2 diabetes. The Verona Diabetes Study. Diabetes Care 1999;22:756-761.
- EASL–EASD–EASO Clinical Practice Guidelines for the management of nonalcoholic fatty liver disease. J Hepatol 2016;64:1388-1402.
- Dulai PS, et al. Increased risk of mortality by fibrosis stage in nonalcoholic fatty liver disease: Systematic review and meta-analysis. Hepatology 2017;65:1557-1565.
- Ruhl CE, Everhart JE. Relationship of non-alcoholic fatty liver disease with cholecystectomy in the US population. Am J Gastroenterol 2013;108:952-958.
- Rinella ME. Nonalcoholic fatty liver disease: A systemic review. JAMA 2015;313:2263-2273.
- Leite NC, et al. Prevalence and associated factors of non-alcoholic fatty liver disease in patients with type-2 diabetes mellitus. Liver Int 2009;29:113-119.
- Prashanth M, et al. Prevalence of nonalcoholic fatty liver disease in patients with type 2 diabetes mellitus. J Assoc Physicians India 2009;57:205-210.
- Assy N, et al. Fatty infiltration of liver in hyperlipidemic patients. Dig Dis Sci 2000;45:1929-1934.
- Boza C, et al. Predictors of nonalcoholic steatohepatitis (NASH) in obese patients undergoing gastric bypass. Obes Surg 2005;15:1148-1153.
- Amarapurkar D, et al. Prevalence of non-alcoholic fatty liver disease: population based study. Ann Hepatol 2007;6:161-163.
- Patell R, et al. Non-alcoholic fatty liver disease (NAFLD) in obesity. J Clin Diagn Res 2014;8:62-66.
- Fracanzani AL, et al. Risk of severe liver disease in NAFLD with normal aminotransferase levels: A role for insulin resistance and diabetes. Hepatology 2008;48:792-798.
- Chou R, Wasson N. Blood tests to diagnose fibrosis or cirrhosis in patients with chronic hepatitis C virus infection: A systematic review. Ann Intern Med 2013;158:807-820.
- Chalasani N, et al. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Disease. Hepatology 2018;67:328-357.
- Musso G, et al. Impact of current treatments on liver disease, glucose metabolism and cardiovascular risk in non-alcoholic fatty liver disease (NAFLD): A systematic review and meta-analysis of randomized trials. Diabetologia 2012;55:885-904.
- Vilar-Gomez E, et al. Weight loss through lifestyle modification significantly reduces features of nonalcoholic steatohepatitis. Gastroenterology 2015;149:367-378.
- Fontana L, et al. Long-term calorie restriction is highly effective in reducing the risk for atherosclerosis in humans. Proc Natl Acad Sci U S A 2004;101:6659-6663.
- Kirk E, et al. Dietary fat and carbohydrates differentially alter insulin sensitivity during caloric restriction. Gastroenterology 2009;136:1552-1560.
- Haufe S, et al. Randomized comparison of reduced fat and reduced carbohydrate hypocaloric diets on intrahepatic fat in overweight and obese human subjects. Hepatology 2011;53:1504-1514.
- St. George A, et al. Independent effects of physical activity in patients with nonalcoholic fatty liver disease. Hepatology 2009;50:68-76.
- Sung KC, et al. Effect of exercise on the development of new fatty liver and the resolution of existing fatty liver. J Hepatol 2016;65:791-797.
- Sjostrom L, et al. Bariatric surgery and long-term cardiovascular events. JAMA 2012;307:56-65.
- Pontiroli AE, Morabito A. Long-term prevention of mortality in morbid obesity through bariatric surgery. A systematic review and meta-analysis of trials performed with gastric banding and gastric bypass. Ann Surg 2011;253:484-487.
- Adams TD, et al. Long-term mortality after gastric bypass surgery. N Engl J Med 2007;357:753-761.
- Sjostrom L, et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med 2007;357:741-752.
- Marchesini G, et al. Metformin in non-alcoholic steatohepatitis. Lancet 2001;358:893-894.
- Uygun A, et al. Metformin in the treatment of patients with nonalcoholic steatohepatitis. Aliment Pharmacol Ther 2004;19:537-544.
- Nair S, et al. Metformin in the treatment of non-alcoholic steatohepatitis: A pilot open label trial. Aliment Pharmacol Ther 2004;20:23-28.
- Li Y, et al. Metformin in nonalcoholic fatty liver disease: A systematic review and meta-analysis. Biomed Rep 2013;1:57-64.
- Musso G, et al. A meta-analysis of randomized trials for the treatment of nonalcoholic fatty liver disease. Hepatology 2010;52:79-104.
- Soccio RE, et al. Thiazolidinediones and the promise of insulin sensitization in type 2 diabetes. Cell Metab 2014;20:573-591.
- Ratziu V, et al. Rosiglitazone for nonalcoholic steatohepatitis: One-year results of the randomized placebo controlled Fatty Liver Improvement with Rosiglitazone Therapy (FLIRT) trial. Gastroenterology 2008;135:100-110.
- Ratziu V, et al. Long-term efficacy of rosiglitazone in nonalcoholic steatohepatitis: Results of the fatty liver improvement by rosiglitazone therapy (FLIRT 2) extension trial. Hepatology 2010;51:445-453.
- Hiatt WR, et al. The cardiovascular safety of diabetes drugs — insights from the rosiglitazone experience. N Engl J Med 2013;369:1285-1287.
- Belfort R, et al. A placebo-controlled trial of pioglitazone in subjects with nonalcoholic steatohepatitis. N Engl J Med 2006;355:2297-2307.
- Cusi K, et al. Long-term pioglitazone treatment for patients with nonalcoholic steatohepatitis and prediabetes or type 2 diabetes mellitus: A randomized trial. Ann Intern Med 2016;165:305-315.
- Aithal GP, et al. Randomized, placebo-controlled trial of pioglitazone in nondiabetic subjects with nonalcoholic steatohepatitis. Gastroenterology 2008;135:1176-1184.
- Eguchi Y, et al. Pilot study of liraglutide effects in non-alcoholic steatohepatitis and non-alcoholic fatty liver disease with glucose intolerance in Japanese patients (LEAN-J). Hepatol Res 2015;45:269-278.
- Armstrong MJ, et al. Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN): A multicentre, doubleblind, randomised, placebo-controlled phase 2 study. Lancet 2016;387:679-690.
- Armstrong MJ, et al. Safety and efficacy of liraglutide in patients with type 2 diabetes and elevated liver enzymes: Individual patient data meta-analysis of the LEAD program. Aliment Pharmacol Ther 2013;37:234-242.
- Kenny PR, et al. Exenatide in the treatment of diabetic patients with non-alcoholic steatohepatitis: A case series. Am J Gastroenterol 2010;105:2707-2709.
- Vizuete J, et al. Perspectives on nonalcoholic fatty liver disease: An overview of present and future therapies. J Clin Transl Hepatol 2017;5:67-75.
- Harrison SA, et al. Orlistat for overweight subjects with nonalcoholic steatohepatitis: A randomized, prospective trial. Hepatology 2009;49:80-86.
- Zelber-Sagi S, et al. A double-blind randomized placebo-controlled trial of orlistat for the treatment of nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol 2006;4:639-644.
- El-Serag HB, et al. Statins are associated with a reduced risk of hepatocellular carcinoma in a large cohort of patients with diabetes. Gastroenterology 2009;136:1601-1608.
- Chatrath H, et al. Dyslipidemia in patients with nonalcoholic fatty liver disease. Semin Liver Dis 2012;32:22-29.
- Sumida Y, et al. Involvement of free radicals and oxidative stress in NAFLD/NASH. Free Radic Res 2013;47:869-880.
- Sumida Y, et al. Serum thioredoxin levels as a predictor of steatohepatitis in patients with nonalcoholic fatty liver disease. J Hepatol 2003;38:32-38.
- Miller ER, et al. Meta-analysis: High-dosage vitamin E supplementation may increase all-cause mortality. Ann Intern Med 2005;142:37-46.
- Sumida Y, Yoneda M. Current and future pharmacological therapies for NAFLD/NASH. J Gastroenterol 2017;53:362-376.
- Staels B, et al. Hepatoprotective effects of the dual peroxisome proliferator-activated receptor alpha/delta agonist, GFT505, in rodent models of nonalcoholic fatty liver disease/nonalcoholic steatohepatitis. Hepatology 2013;58:1941-1952.
- Ratziu V, et al; GOLDEN-505 Investigator Study Group. Elafibranor, an agonist of the peroxisome proliferator-activated receptor-a and -d, induces resolution of nonalcoholic steatohepatitis without fibrosis worsening. Gastroenterology 2016;150:1147-1159.
- Ishibashi S, et al; K-877-04 Study Group. Effects of K-877, a novel selective PPARa modulator (SPPARMa), in dyslipidaemic patients: A randomized, double blind, active- and placebo-controlled, phase 2 trial. Atherosclerosis 2016;249:36-43.
- Honda Y, et al. Pemafibrate, a novel selective peroxisome proliferator-activated receptor alpha modulator, improves the pathogenesis in a rodent model of nonalcoholic steatohepatitis. Sci Rep 2017;7:42477.
- Neuschwander-Tetri BA, et al; NASH Clinical Research Network. Farnesoid 9 nuclear receptor ligand obeticholic acid for non-cirrhotic, non-alcoholic steatohepatitis (FLINT): A multicentre, randomised, placebo-controlled trial. Lancet 2015;385:956-965.
- Safadi R, et al; FLORA Group. The fatty acid-bile acid conjugate Aramchol reduces liver fat contentin patients with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol 2014;12:2085-2091.
- Brenner C, et al. Decoding cell death signals in liver inflammation. J Hepatol 2013;59:583-594.
- Barreyro FJ, et al. The pan-caspase inhibitor Emricasan (IDN-6556) decreases liver injury and fibrosis in a murine model of nonalcoholic steatohepatitis. Liver Int 2015;35:953-966.
- Mizrahi M, et al. Alleviation of insulin resistance and liver damage by oral administration of Imm124-E is mediated by increased Tregs and associated with increased serum GLP-1 and adiponectin: Results of a phase I/II clinical trial in NASH. J Inflamm Res 2012;5:141-150.
- Henderson NC, Sethi T. The regulation of inflammation by galectin-3. Immunol Rev 2009;230:160-171.
- National Institute of Diabetes and Digestive and Kidney Diseases. Eating, Diet, & Nutrition for NAFLD and NASH. Available at: https://www.niddk.nih.gov/health-information/liver-disease/nafld-nash/eating-diet-nutrition. Accessed Feb. 23, 2018.
- American Liver Foundation. Non-Alcoholic Fatty Liver. Disease Available at: https://www.liverfoundation.org/for-patients/non-alcoholic-fatty-liver-disease/#1503447887129-f4b80b1f-978a. Accessed Feb. 23, 2018.
- Imbert-Bismut F, et al. Biochemical markers of liver fibrosis in patients with hepatitis C virus infection: A prospective study. Lancet 2001;357:1069-1075.
- Halfon P, et al. A prospective assessment of the inter-laboratory variability of biochemical markers of fibrosis (FibroTest) and activity (ActiTest) in patients with chronic liver disease. Comp Hepatol 2002;1:3.
- Naveau S , et al. Diagnostic and prognostic values of noninvasive biomarkers of fibrosis in patients with alcoholic liver disease. Hepatology 2009;49:97-105.
- Angulo P, et al. Simple noninvasive systems predict long-term outcomes of patients with nonalcoholic fatty liver disease. Gastroenterology 2013;145(4):782-789.
- Angulo P, et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007;45:846-854.
- Cichoż-Lach H, et al. The BARD score and the NAFLD fibrosis score in the assessment of advanced liver fibrosis in nonalcoholic fatty liver disease. Med Sci Monit 2012;18:CR735-CR740.
Nonalcoholic fatty liver disease (NAFLD) is the most common liver pathology worldwide and is the third leading cause of liver transplantation in the United States.This article reviews the pathogenesis, diagnosis, and natural history of NAFLD as well as known treatments and future therapies.
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.